As the need for accessible living environments grows, Environmental Control Units (ECUs) emerge as pivotal tools in occupational therapy. These electronic devices empower individuals with significant physical impairments by helping them control their surroundings, thus enhancing their independence and improving quality of life. In this article, we will delve into the fundamentals of ECUs, explore the essential role occupational therapists play in their integration, examine technological innovations shaping these units, and address the critical aspects of funding and accessibility that influence their usage. Together, these topics highlight the necessity of ECUs in supporting those striving for autonomy and social engagement.
Quiet Autonomy: Reclaiming Daily Life Through Environmental Control Units in Occupational Therapy

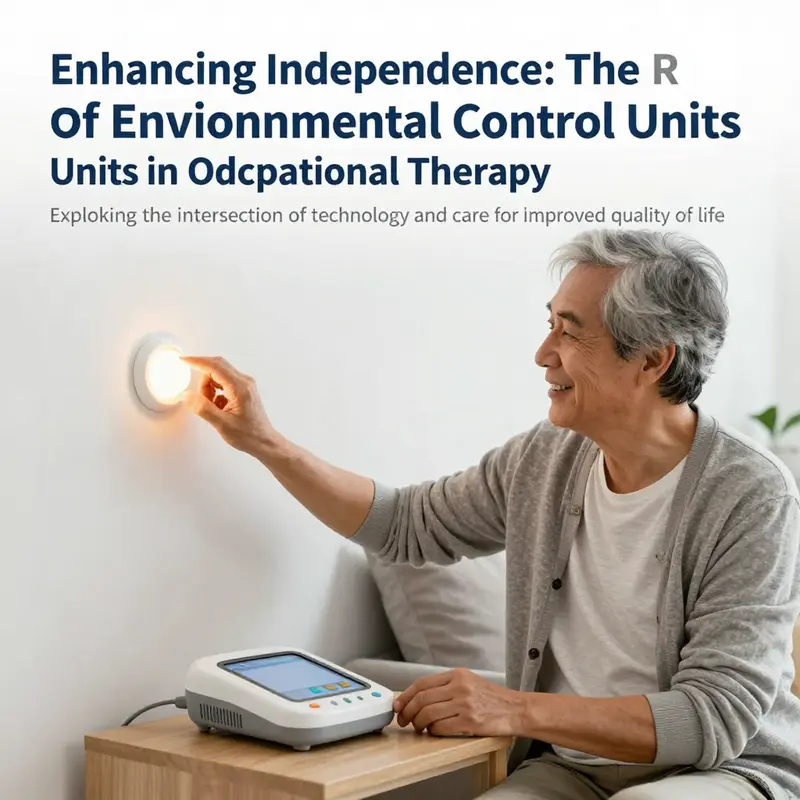
Environmental Control Units, or ECUs, are more than gadgets designed to press a few buttons from a chair or bed. They are instruments of autonomy tailored to people who experience significant physical impairment that limits the use of upper and/or lower limbs. In occupational therapy, ECUs translate a clinician’s aim to restore meaningful participation into practical, daily occurrences. They enable a client to regulate lighting to suit mood and activity, adjust heating for comfort, operate kitchen appliances to prepare meals, and even manage communication devices to stay connected with family, friends, and support networks. The essence of ECUs lies in their capacity to reframe what a person can reasonably accomplish despite a loss of motor control, thereby redefining the boundaries between dependence and independent living. In the clinical conversations that drive therapy, ECUs are not merely assistive devices; they are pathways to self-determination, crafted through careful assessment, training, and integration into the home and community environment.
The need for environmental control arises when a long-term physical impairment disrupts the ability to perform everyday tasks that make a person self-sufficient. In England, NHS guidance and current professional literature emphasize that ECUs are prescribed for individuals whose impairment stems from disease, trauma, or congenital conditions resulting in reduced functional movement. The impairment must be physical in nature to qualify for environmental control funding under traditional pathways. Purely sensory limitations, such as vision loss, are typically addressed through separate support streams. This boundary—physical impairment as the criterion for ECU funding—reflects how ECUs situate themselves at the intersection of rehabilitation science, technologic innovation, and health-system funding frameworks. The practical implication for practitioners is clear: ECUs must be considered in the broader context of mobility, dexterity, and the person’s goals for participation in daily life.
Historically, ECUs were austere in form, focused on enabling basic environmental manipulation. Over the past several decades, their scope has broadened dramatically. Traditional systems were mostly single-purpose and device-centric, designed to manage one or two tasks within the immediate environment. Today, the lines between ECUs and mainstream technology have blurred. Modern ECUs increasingly incorporate connectivity features that link the physical environment to digital ones. A user may now navigate computer technologies, access online services, and engage in social communication through the same control interface that toggles a lamp or opens a door. This evolution mirrors a shift in occupational therapy toward holistic rehabilitation, where independence is not only about controlling lights and doors but about participating in digital life, maintaining social ties, and sustaining mental well-being.
Classification, regulation, and the evolving scope of ECUs are not abstract concerns; they shape what therapists can prescribe, how funding is secured, and how care pathways are designed. Traditionally, ECUs have been categorized as medical devices, with many systems classified as Class 1 under EU regulations. That status reflects a baseline of safety and consumer-grade complexity, allowing clinicians to integrate ECU technology into home and therapy settings with established risk management practices. Yet the rapid integration of mainstream devices—such as smartphones, tablets, and internet-enabled ecosystems—suggests that regulatory categories may adapt as capabilities multiply. The regulatory conversation, historically anchored in device safety and basic functionality, increasingly centers on interoperability, user-centric design, and data privacy. For practitioners, this means staying informed about evolving standards and ensuring that the intended use of ECUs aligns with current guidelines while still satisfying individual rehabilitation goals.
The expanding reach of ECUs into virtual environments marks a significant turning point in practice. No longer confined to controlling the lamp in a living room, ECUs now offer pathways to computer literacy, online communication, and digital social engagement. Occupational therapists find themselves guiding clients toward meaningful participation in virtual communities, telehealth, and remote work or study, as appropriate. In the United Kingdom, NHS environmental control services have started to reflect this broader remit, with supports that cover access to computer technologies and online platforms alongside traditional environmental management. This shift is not merely about convenience; it is about inclusion. When people can communicate with others, access information, and participate in online activities, their sense of agency grows, and mental health and quality of life often improve alongside physical function. The ECU, then, becomes a bridge that connects physical capability to social capital.
From a practice perspective, ECUs demand a thorough, client-centered assessment process. Occupational therapists begin by mapping a person’s goals: what daily activities matter most, what safety considerations exist in the home, and which tasks, if enabled, would broaden participation. The assessment probes not only the person’s current motor abilities but also their preferred modes of interaction. Some clients rely on residual movement and prefer switch-activated controls; others benefit from voice-controlled interfaces; yet others come to rely on eye-gaze or head-tracking systems when limb movement is severely limited. The selection of an ECU is therefore highly individualized, grounded in a careful analysis of motor capability, cognitive load, sensory access, and the home’s physical layout. The environment itself becomes a partner in therapy: doorways, lighting placements, appliance locations, and furniture arrangements are all considered to optimize accessibility and safety.
In therapy rooms and in families’ living spaces, the process of introducing an ECU unfolds as a collaboration. The therapist educates clients and caregivers about how ECUs operate, what their limits are, and how to troubleshoot common issues. This education includes training on email alerts, device pairing, and routine maintenance to prevent frustration or disengagement. It also involves risk assessment, ensuring that users can confidently operate emergency features, alarms, and climate controls, while maintaining safety in potentially risky areas like the kitchen or bathroom. Training is not a one-off event but an ongoing partnership that supports gradual skill acquisition, confidence-building, and, crucially, adaptability. A key outcome a therapist aims for is not simply the successful execution of a series of tasks but the emergence of a durable sense of independence. The client learns to choose when to use the ECU, what to automate, and how to modify routines as needs change or as new technologies become available.
The practical realization of ECU-enabled independence is not just about devices but about the integration of those devices into a daily life rhythm. Therapists work closely with clients to configure systems so that they respond predictably to the person’s routines. For example, a client who wakes early might rely on a sequence that turns on lights, prepares the coffee machine via a voice command, and opens the blinds to invite daylight, all before stepping into the kitchen. Later, the same program might adjust room temperature or cue the television to display familiar information, thereby reducing cognitive load. The efficiency of these routines can dramatically reduce reliance on caregivers, freeing both clients and families to participate in activities that were previously impractical or exhausting. The relationship between ECUs and psychological well-being cannot be overstated. When a person feels more in control, anxiety can lessen, mood may improve, and engagement in meaningful occupations—such as preparing meals, managing personal care, or communicating with loved ones—becomes more consistent.
As therapists guide clients through the initial setup, they also consider the broader ecosystem of care. Interdisciplinary collaboration is essential. OT teams may coordinate with engineers, speech and language therapists, physiotherapists, and social workers to tailor ECU solutions that fit medical needs, home environments, and community resources. In some cases, ECUs must adapt to evolving mobility strategies or intersect with rehabilitation technologies, such as computer-access software or smart home ecosystems. The goal is not only to restore function within specific tasks but also to empower the individual to participate in life as a whole—from daily chores to social engagement and self-advocacy within the health and social care system. In this sense, ECUs become a strategic component of a person’s overall rehabilitation plan, rather than a standalone intervention.
An important nuance in practice concerns funding pathways and eligibility. The NHS and other public bodies often frame ECU provision within specific medical-device categories and pathways. Sensory impairments like vision loss are typically managed through separate avenues, so ECUs focus on motor impairment and functional movement loss. This distinction does not diminish the value of ECUs; it rather clarifies routes for access and reimbursement. Therapists must navigate policy landscapes with clients and families, advocating for needed supports while ensuring compliance with regulatory requirements. By communicating the rationale behind selecting a particular ECU configuration, therapists help clients understand how interventions align with both short-term goals and long-term plans for living well with disability. The knowledge that ECUs are embedded in a regulated framework can be reassuring for families, yet it also underscores the need for ongoing professional guidance as technology evolves.
The clinical narrative of ECUs today blends practical technical capability with a deeply human understanding of daily life. Clients are not only learning to press a button or speak a command; they are re-structuring their day around an environment that responds to them rather than requiring the user to adapt to the environment. The therapeutic value of ECUs extends beyond functional independence. By enabling access to digital literacy, online communication, and even social participation, ECUs help counter the social isolation that can accompany long-term physical disability. When a client can participate in a video call, manage an email, or collaborate on a shared digital document, the sense of belonging and purpose often strengthens, creating a positive feedback loop that supports motivation, engagement, and rehabilitation momentum.
The conversation about ECUs also invites reflection on what counts as meaningful participation. Occupational therapy prioritizes activities that matter to the individual—the day-to-day tasks that sustain independence, the social rituals that provide connection, and the goals that give life structure and dignity. ECUs realize this philosophy in tangible form. They are not merely about extending the range of motions or preserving energy; they are about enabling a person to decide what to do with a day, how to do it, and with whom. In that sense, ECUs are aligned with core occupational therapy principles: person-centered practice, participation in meaningful activities, and optimization of independence within the constraints of impairment. The practice of selecting, configuring, and teaching ECUs thus becomes an exercise in empathy as much as an exercise in engineering.
For clinicians seeking practical inspiration that links ECU practice to broader therapeutic aims, resources that illustrate how technology supports rehabilitation are valuable. In particular, the way occupational therapy aids integrate with recovery processes for stroke survivors offers a relevant frame for ECUs in other motor impairments. This connection helps clinicians think through how to adapt ECU configurations to changing motor patterns, cognitive demands, and fatigue levels that often accompany neurological recovery. By considering stroke recovery as a lens, therapists can extrapolate principles such as graded exposure to new interfaces, the pacing of skill acquisition, and the importance of meaningful, goal-directed practice when introducing ECUs into a client’s routine. The continuity from acute to chronic care becomes clearer when ECUs are positioned as a bridge between physical capacity and the social world that gives daily life shape and meaning. As practice evolves, therapists remain attentive to safety, usability, and the need to preserve dignity by honoring the person’s preferences and pace.
The evidence base for ECUs, like many prosthetic and assistive technologies, is continually expanding. Systematic reviews, clinical guidelines, and professional discourse emphasize that ECUs should be selected to fit the individual’s unique constellation of abilities, environments, and goals. The dialogue around ECUs also encourages clinicians to consider regulatory and ethical dimensions, including data privacy, device management, and user autonomy. In a world where technology becomes increasingly integrated into health care, the practitioner’s role is to translate complex technical options into accessible, person-centered solutions. The chapter’s evolving landscape—where a single switch or voice command can initiate a cascade of actions across a home—illustrates how occupational therapy adapts to technological progress while preserving core professional values.
As part of ongoing professional development, clinicians often consult broader resources to ground their practice in current evidence and policy. The British Journal of Occupational Therapy has featured reviews and discussions that anchor the ECU concept within contemporary rehabilitation practice, highlighting the need for personalized assessment, appropriate training, and robust home adaptation strategies. The dialog between research and practice helps ensure that ECU interventions remain scientifically grounded while responsive to patient and family experiences. Clinicians are reminded that ECUs are not static devices; they are dynamic tools that require regular re-evaluation as needs shift, as home environments change, and as newer technologies become accessible. The ultimate objective remains consistent: empower individuals to live with greater autonomy, reduce reliance on direct care, and foster social inclusion through intentional, technologically supported engagement with the world around them.
In closing, the narrative of environmental control in occupational therapy is a narrative of liberation through design. It is about turning the physical constraints of disability into opportunities for independence, for social connection, and for lifelong learning. ECUs embody a therapeutic philosophy that honors personhood and choice, offering a practical means to translate intention into action in everyday life. They invite therapists, clients, and families into a shared enterprise—shaping environments, building skills, and cultivating confidence in the capability to influence one’s surroundings. The result is not merely a smoother daily routine but a more vibrant sense of belonging, a greater willingness to try new activities, and a deeper conviction that participation in life remains possible, even in the face of significant impairment. For practitioners who want to bridge clinical insight with lived experience, ECUs stand as a compelling reminder that technology, when aligned with person-centered care, can expand the horizons of what a person can do—and who they can be—in their own home and in their broader community.
For practitioners seeking practical examples of how occupational therapy aids can support broader recovery and activity engagement, see OT aids in stroke recovery. This resource illustrates how assistive technologies and therapeutic strategies intersect to promote meaningful participation across the continuum of care. The principle remains the same when applying ECU strategies: tailor technology to the person, align tasks with real-life goals, and support gradual, confident progression toward greater independence. As care pathways continue to evolve within NHS services and beyond, ECUs offer a flexible, humane approach to rehabilitation that honors both the science of motor recovery and the art of living well with disability. Further reading and continued professional dialogue help ensure that ECU practice remains current, ethical, and deeply attentive to the person at the center of every therapeutic decision.
External references and further reading provide essential context for clinicians and researchers alike. An authoritative overview of ECU use and its implications for occupational therapy—along with contemporary regulatory considerations—can be found in the British Journal of Occupational Therapy (2026). To delve into the clinical application and evidence base, see the comprehensive review by Sheelagh Richards in the journal. This work situates ECUs within a broader rehabilitation framework, linking device selection, training, and home integration to outcomes such as independence, participation, and psychological well-being. The evolution of ECUs—from basic environmental controls to connected systems capable of interfacing with virtual environments—mirrors the trajectory of occupational therapy toward more holistic, inclusive care that embraces technology as an ally rather than a barrier.
Further reading: https://doi.org/10.1177/03080226261123456
Internal link for practitioners: OT aids in stroke recovery
Architects of Independence: How Occupational Therapists Implement Environmental Control Units

Environmental Control Units (ECUs) do more than replace a switch; they translate intention into action, turning a moment of need into the ability to respond to a living space. In the field of occupational therapy, ECUs sit at the intersection of function, technology, and daily life. They are not merely devices; they are enablers of autonomy that demand a careful, person-centered approach to match the right tool to the person, the home, and the rhythm of daily routines. The chapter examines the critical role occupational therapists play in selecting, implementing, and sustaining ECU use, drawing on evidence from rehabilitation literature that situates therapists at the core of assessment, planning, and training.
In the classic literature, a 1997 study by S. A. Holme reported a striking finding: in the surveyed facilities, the vast majority of respondents—about 88 percent—identified occupational therapists as the primary professionals responsible for evaluating and recommending ECUs. That statistic, though dated, reveals a long-standing consensus about the OT’s unique expertise in bridging functional assessment with environmental modification. It underscores a professional identity built on understanding not only what a person can do but how the surrounding environment can be shaped to support what they want to do. The OT is trained to look at the person in context—grasping how cognitive sequencing, motor control, sensory processing, and emotional state interact with a person’s tasks such as lighting a room, turning on a heater, answering a phone, or enabling access to a computer. The ECU is thus not a stand-alone gadget; it is a structured, adaptive system that requires careful calibration to the user’s capabilities and living situation.
A comprehensive assessment is the linchpin of successful ECU intervention. It begins with a clear exploration of what the user wants to accomplish in daily life, followed by a detailed appraisal of the user’s abilities across several domains: motor control, communication, problem-solving, and attention. The therapist translates those insights into a practical map of tasks that the ECU must support. Are lights controlled with a single switch, or can the user sequence multiple functions in a reliable order? Is a telephone accessible through touch, voice, or an eye-gaze interface? How does the user manage appliances, curtains, or window shades? What happens in the home at different times of day when fatigue or cognitive demands change? The OT also evaluates safety concerns: the risks of misconnections, misfiring commands, or overreliance on the device that could lead to social withdrawal if the user cannot access the environment without the ECU. The aim is to maximize independence while maintaining safety and social participation.
The process, however, extends far beyond device testing. It embodies a holistic, person-centered framework that sees ECUs as part of a broader rehabilitation plan. Occupational therapists work within a multidisciplinary team that often includes physiatrists, physical therapists, speech-language pathologists, social workers, and information technology specialists. The collaboration mirrors the complexity of modern rehabilitation, where motor recovery, cognitive function, and social participation are interwoven. This team-based model ensures that the ECU aligns with medical stability, mobility capabilities, communication needs, and the patient’s psychosocial goals. The OT coordinates these threads, ensuring that the technology is not an isolated intervention but an integrated support that harmonizes with therapy, home care routines, and the user’s personal aspirations.
As ECUs have evolved, so too has the scope of what they can connect to and how they can be controlled. Traditional systems were primarily stand-alone devices that offered basic control over lights, doors, or simple appliances. Today’s ECUs often incorporate connectivity that allows users to engage with virtual environments, online services, and digital communication platforms. This expansion is particularly meaningful in rehabilitation, where social inclusion and access to information are essential for psychological well-being and ongoing motivation. When an OT plans an ECU, they consider not only immediate physical access but also the user’s engagement with the digital world—telehealth, messaging with family, online banking, or attending virtual support groups. The modern ECU therefore becomes a bridge between the home and the wider world, supporting not just autonomy but meaningful participation in daily life.
In England and elsewhere, funding and regulatory frameworks have historically treated ECUs as medical devices, often categorized as Class 1 under traditional EU regulations. This classification has shaped procurement pathways and the level of clinical oversight required for prescription and reimbursement. Yet the regulatory landscape is shifting as mainstream technologies—smartphones, tablets, and internet-connected home devices—enter the ecosystem. The result is a gradual rethinking of how ECUs are classified and reimbursed, a shift that places the OT at the center of translating clinical need into accessible technology. The OT’s role becomes especially vital when technologies cross into consumer devices that require calibration, accessibility settings, and safety considerations unique to each user. The aim remains constant: ensure that devices are medically appropriate, safe to use, and capable of evolving with the person’s changing needs.
An OT-led ECU plan begins in the home environment, where the person’s routines, spatial layout, and caregiver supports shape what is possible. The home is the primary stage for integration, and therapists often perform in-situ assessments that reveal issues not evident in clinic settings. For example, a corridor with a narrow turn might require a particular switch placement, or a switch’s reach might be limited by postural changes after surgery or a progressive condition. The therapist’s eye for these details helps determine the most appropriate control method—switch-activated, voice-controlled, or eye-gaze operated—and how it will be positioned, labeled, and tested to ensure reliable performance. Training is a cornerstone of success. The OT leads hands-on sessions with the user and caregivers, teaching operation sequences, contingency plans for power outages or device failures, and the steps needed to maintain safety. They also educate on how to adjust the ECU for new tasks as the person’s goals shift, such as enabling videoconferencing for social connections, which can become a vital source of emotional support and cognitive engagement. Therapists also point clients toward practical toolkits and equipment resources that support everyday practice; for example, Tools and Equipment for Occupational Therapists offers a concise reference for aligning device choices with daily routines.
The selection process is nuanced. It requires balancing ease of use with reliability, speed of response with cognitive load, and cost with long-term value. A single neat arrangement rarely suffices; more often, therapists tailor combinations of controls to create redundancy. For instance, a user might have a primary voice control but also a secondary switch to mitigate the risk of misinterpretation by a voice interface during a stressful moment. The OT considers how the user’s environment will change with seasons, visitor patterns, or travel, and anticipates how the ECU must adapt. In some cases, the ECU will function as a gateway to broader digital access, enabling the user to operate a computer or tablet to send messages, browse information, or participate in online communities. This expanded scope is not incidental. It is aligned with contemporary rehabilitation goals that emphasize social participation, self-efficacy, and autonomy as multidimensional outcomes.
A critical component of an OT’s practice is ongoing troubleshooting and refinement. ECUs are not one-off solutions but living systems that require periodic reprogramming, reconfiguration, and sometimes hardware updates as user needs evolve. Occupational therapists monitor usage patterns, solicit feedback from users and caregivers, and adjust settings to reduce fatigue, prevent errors, and maintain motivation. They may also troubleshoot issues that arise from the intersection of medical devices with living spaces—ensuring that wiring is unobtrusive, that devices are safe around children or pets, and that users have access to support for software updates. The aim is a sustainable intervention: a system that remains aligned with the user’s evolving goals, fits within the home environment, and reduces reliance on external care without compromising safety or well-being.
Within the NHS and other health systems, ECUs have become a central component of rehabilitation programs. They are positioned not only as a means to operate lights and appliances but as a gateway to independent living and digital inclusion. When therapists design ECU interventions in the NHS context, they consider the patient’s broader rehabilitation trajectory, including cognitive training, mobility, and social participation. They collaborate with other clinicians to ensure that the ECU supports therapeutic activities that may occur in daily living, such as cooking or laundry, while also enabling access to online resources, telecommunication, or community services. The result is a holistic intervention that supports both physical independence and social connectedness, enabling individuals to engage with their communities rather than retreat from them.
The practice also invites reflection on equity and accessibility. Sensory impairments, such as vision loss, may present access barriers to environmental controls. Although vision impairment is not typically funded through the same ECU pathways, therapists are trained to consider alternative access methods and to propose adaptations that preserve the user’s independence. They also advocate for inclusive design in the home and community environments, supporting clients in navigating stairs, thresholds, and other barriers. This is where the OT’s expertise in activity analysis—evaluating the demands of tasks and the strategies that best meet them—becomes a tool for social justice, ensuring that people with different strengths and limitations can participate meaningfully in daily life.
The integration of ECUs into rehabilitation practice also has implications for clinical training and professional development. Therapists require a blend of clinical acumen, technical literacy, and user-centered communication skills. They must stay current with evolving technologies while maintaining a critical eye for safety, usability, and evidence of efficacy. Professional development may include training in human-computer interaction, assistive technology application, and the assessment of cognitive strategies that support device use. This ongoing learning is essential, given how rapidly assistive technologies change and how patient needs may shift with disease progression or aging. In supporting this development, the OT cultivates relationships with manufacturers, technicians, and digital health teams, translating clinical needs into practical hardware and software configurations that can be implemented in clinics and homes.
Implementation science also informs how ECUs are prescribed and sustained in real-world settings. The transfer from clinic to home hinges on user-friendly training materials, clear care plans, and robust caregiver support. Therapists design stepwise practice routines that align with daily schedules, offer fallback options, and anticipate moments of frustration. They may create simple visual prompts or labeled control layouts that help users master the system with confidence. They also consider cultural and linguistic factors, ensuring that training materials are accessible and respectful of the user’s background. All of these elements contribute to the ECU not simply as a device, but as an integrated part of daily living.
For those seeking further reading on the topic, a detailed overview of environmental control systems can be found in authoritative medical literature. The chapter on environmental control systems in the NCBI Bookshelf provides foundational insight into how ECUs function, how to assess and prescribe them, and how longitudinal management within rehabilitation settings can be designed for durability and effectiveness. This resource helps frame the OT’s role within a broader evidence base and offers guidance for future research that can enhance practice. Link: https://www.ncbi.nlm.nih.gov/books/NBK562340/
In closing, occupational therapists occupy a pivotal position in the story of ECUs. They translate technical possibilities into meaningful, everyday actions, enabling people with significant physical disabilities to shape their own environments and, by extension, their lives. The OT’s work with ECUs is not just about controlling devices; it is about enabling participation, protecting dignity, and supporting mental health through autonomy. The chapter of practice that centers ECUs demonstrates how rehabilitation is built not only on restoring function but on crafting environments that reflect the person’s goals, preferences, and social context. When done well, ECU integration redefines what is possible for a person in a wheelchair, a user with limited dexterity, or anyone whose mobility constrains traditional interaction with daily surroundings.
To support clinicians and researchers seeking practical resources, it is helpful to consider how OT practice sits alongside the broader literature on assistive technology and environmental modification. The evidence suggests that the most successful ECUs are those chosen and configured through a collaborative process that honors the client’s values and life context, rather than a one-size-fits-all solution. In that spirit, therapists who work in rehabilitation should maintain an ongoing dialogue with users, families, and care networks, revisiting goals as abilities and environments change. They should also remain vigilant for opportunities to expand access to digital services and social participation, recognizing that independence is not merely about moving through a doorway but about moving toward fuller engagement with the world.
For readers seeking more technical grounding, the NHS and academic literature emphasize the importance of task analysis, individualized goal setting, and outcome measurement in ECU programs. The practice hinges on careful observation, iterative testing, and patient-focused adjustments that reflect the user’s evolving capacities. The chapter by Holme and subsequent research reinforce the centrality of the occupational therapist in ECU prescription, integration, and follow-up. In keeping with the evidence base, the profession continues to refine its approaches to ensure that ECUs meet the highest standards of safety, reliability, and user satisfaction, while also pushing toward a broader integration with mainstream digital ecosystems that can support both physical independence and social connection.
Further reading and resources, including practical guides and research syntheses, complement clinical training by providing case studies, device considerations, and strategies for long-term management. The interface between clinical care and technology is dynamic, and the OT’s expertise in assessment, adaptation, and education remains essential in guiding this evolution. The result is a rehabilitation landscape in which ECUs contribute to a broader vision of person-centered care—one that respects autonomy, preserves dignity, and promotes life-enhancing participation in home, work, and community life.
In sum, the role of occupational therapists in implementing ECU technology is characterized by a combination of rigorous clinical assessment, collaborative care, patient education, and thoughtful adaptation of both devices and environments. This integrative approach yields outcomes that extend beyond immediate convenience, reaching toward enhanced independence, reduced caregiver burden, and improved psychological well-being. The OT’s leadership in ECU planning and execution thus stands as a powerful testament to the profession’s commitment to enabling people to live with agency in the contexts that matter most to them.
- End of chapter.
From Switches to Synapses: How Environmental Control Units Reframe Occupational Therapy and Everyday Independence

Environmental Control Units (ECUs) have long stood as quiet allies in rehabilitation, quietly expanding the horizons of what people can do when their bodies no longer cooperate with standard controls. In occupational therapy, ECUs are more than devices; they are translated possibilities, turning impairment into capacity and constraint into choice. The evolution of ECUs mirrors a broader shift in care philosophy: independence is not merely about performing tasks, but about being able to participate in the rhythms of daily life with dignity and purpose. In England, the clinical and funding landscapes shape how ECUs are prescribed, implemented, and supported within the patient’s home and community. Yet the core motivation remains consistent: to help people regain control over their immediate environment—lighting, heating, doors, telecommunication devices—and through that control, to rebuild a sense of agency and self-determination. The therapeutic aim is not to replace human care with circuitry but to harmonize human capability with technology in a way that respects the person’s goals, preferences, and lived experience.
Technological progress has pushed ECUs far beyond their original remit. The earliest systems were simple, junction-based solutions: a user could operate a light or a TV with a switch or a push-button. Today’s ECUs weave wireless connectivity, voice recognition, eye gaze, sensors, and smartphone integration into cohesive ecosystems. This expansion is not merely about convenience; it redefines participation. When a person can raise the blinds, adjust the thermostat, or initiate a video call with a single action, they are not just performing tasks. They are choosing how to spend time, how to manage stress, and how to participate in social and educational life. The NHS England guidelines align with this broader perspective. They recognize ECU provision for individuals whose long-term physical impairment prevents operation of standard hand-controls, and they frame ECUs as medical devices—traditionally Class 1 under EU regulation—while also acknowledging that the regulatory landscape must evolve as mainstream technologies become embedded in care. This regulatory framing matters because it influences funding eligibility, training expectations, maintenance responsibilities, and the safety checks that safeguard users at home. The shift toward integrating ECUs with everyday technology signals a move toward interoperability and user-centered design, reinforcing that devices should adapt to people, not force people to adapt to devices.
The occupational therapy process remains anchored in person-centered assessment, yet it must now contend with a wider array of possibilities. A therapist begins with a holistic view of the client’s living situation: the layout of the home, the proximity of essential devices, the presence of caregivers, and the client’s cognitive and perceptual abilities. The assessment is not a one-off event; it is an ongoing collaboration that evolves as the user gains comfort, as new devices become available, and as the person’s goals shift, whether toward independence in education or re-engagement in work. The therapist examines not only whether a user can operate a light switch, but how they can orchestrate a routine that reduces fatigue and increases predictability. That routine might involve a switch-activated interface for the most reliable moments of motor control, a voice-controlled arrangement when hands are occupied, or an eye-gaze interface when attention to a screen must be preserved while navigating the environment. Each solution is personalized, modular, and prioritized for safety, reliability, and sustainability in the user’s home setting. The training component is essential: users and caregivers must learn to initiate, adapt, and troubleshoot; to understand error patterns; and to reconfigure sequences as the user’s capabilities change. This training goes beyond device operation; it includes strategies for reducing cognitive load, managing environmental distractions, and maintaining attention to safety cues in a complex, multi-device ecosystem. When a client learns to modulate room temperature to promote comfort, to dim lights for a preferred sensory environment, or to access a communication app with ease, the impact extends beyond efficiency. It enriches mood, focus, and willingness to engage in meaningful occupations—studies and social activities, as well as domestic routines. In practice, the ECU is integrated within broader environmental modifications and assistive technologies, forming a resilient system rather than a single, isolated tool. The aim is to ensure that the device complements rather than competes with the person’s existing strengths and compensatory strategies, enabling a smooth transition between different activities across the day. This approach aligns with the contemporary view that ECUs contribute most effectively when embedded in a person’s broader rehabilitation plan that targets participation in daily occupations, social connection, and personal growth.
As ECUs have expanded, so has their ability to facilitate access to digital spaces. The modern ECU is not confined to home lighting and doors; it can enable participation in education, employment, and online social life by providing reliable means to interact with computers, telecommunication platforms, and the internet. The capacity to access online services—digital learning platforms, remote work tools, healthcare portals, and social networks—supports a more inclusive model of rehabilitation. It acknowledges that occupational engagement includes not only physical tasks but also the social and cognitive activities that give life structure and meaning. This emphasis on digital inclusion is particularly important for younger clients who aim to return to school or move into the workforce, and for adults seeking to maintain professional identity and social networks. Yet this broader scope carries responsibilities. Therapists must consider digital literacy, privacy, and cyber safety as integral components of ECU training. They must help clients navigate platforms securely, protect personal information, and avoid fatigue or overwhelm caused by excessive device interdependence. The ethical dimensions of control and autonomy surface here as well: the clinician helps ensure that the user remains the primary decision-maker and that the ECU supports choices rather than dictating them. The regulatory and clinical emphasis on safety, privacy, and user autonomy is not a constraint; it is a framework that clarifies responsibilities, fosters trust, and sustains long-term engagement with the technology. Within this framework,ECUs become enablers of social inclusion and ongoing participation in education and work, which are central to the therapeutic goals of occupational therapy.
From a policy and funding perspective, ECUs sit at the intersection of clinical need, home living realities, and the evolving landscape of assistive technology. NHS services have embraced ECUs as a core component of rehabilitation for individuals with long-term impairments who cannot operate standard controls. The regulatory environment emphasizes the safety and interoperability of devices within health systems, while also recognizing the practical challenge of deploying technology in diverse home contexts. In this light, clinical decisions about ECU prescription balance device capabilities with the user’s home infrastructure, caregiver availability, and budgetary constraints. At times, this balancing act requires creative problem-solving: selecting a robust, straightforward input method when complex multi-modal interfaces might overwhelm a user; coordinating with suppliers to ensure timely maintenance; planning for future upgrades that align with expected changes in function. Importantly, sensory impairments such as vision loss introduce different funding pathways and, if necessary, separate strategies, underscoring the need for a holistic approach to rehabilitation that respects the person’s full sensory and functional profile. A well-conceived ECU plan anticipates changes in function and environment; it favors modular, upgradable components over bespoke, hard-to-maintain configurations. This forward-looking approach helps ensure that people can adapt to evolving needs without repeated, destabilizing device changes. The therapeutic relationship then extends beyond installation and initial training into ongoing support, adjustment appointments, and collaboration with other professionals who contribute to the client’s overall care plan.
The practical and human dimensions of ECU use are inseparable from the people who design, install, and support them. Interdisciplinary teamwork is a hallmark of contemporary rehabilitation, and outcomes improve when therapists, engineers, assistive technology specialists, and caregivers speak a shared language about function, safety, and user experience. The device itself, however sophisticated, remains subordinate to the goal of meaningful occupation and quality of life. The occupational therapist’s expertise in activity analysis, environmental modification, and client-centered coaching guides the choice of input modalities, ensuring they align with a client’s motor capabilities, preferences, and living environment. This is not about chasing the latest feature; it is about building a durable, person-centered solution that can flex as needs evolve. For practitioners seeking to refresh their practice in this area, a practical path is to connect ECU planning with ongoing professional development and collaborative care. See the discussion of interdisciplinary teamwork in occupational therapy here: How do occupational therapists collaborate with other healthcare professionals? This link illustrates how therapists coordinate with nursing, engineering, social work, and education to ensure ECU fits within a holistic care plan. It is a reminder that technology thrives in the hands of teams who understand people, not just devices. The NHS framework that supports access to computer technologies and online services as part of ECU provision reinforces this view, highlighting that technology can extend the reach of therapy beyond clinic walls. In the end, ECUs are about restoring rhythm to life—the tempo of daily routines, the ease of lighting a room at dusk, or the quiet reassurance of a help button in moments of need. The clinician’s task is to harmonize technology with human capacity and desire, to craft a home environment that invites adaptation by design and enables sustained participation in the activities that give life structure, meaning, and shared humanity. For this reason, the chapter you have read is not merely an account of devices; it is a narrative about partnership, resilience, and the practical creativity that makes independence possible in the real world. As ECUs continue to evolve, occupational therapy will increasingly rely on thoughtful assessment, collaborative problem-solving, and a commitment to access—so that people with significant physical impairment can shape their own environments and, in turn, shape their futures.
For current standards and implementation guidance, see NHS England’s mental health guidance: https://www.england.nhs.uk/mental-health/
Opening Doors, Closing Gaps: Funding, Accessibility, and Equity in Environmental Control Units within Occupational Therapy
Environmental Control Units (ECUs) have long stood at the intersection of technology, rehabilitation, and daily living. They translate the complex needs of individuals with significant motor impairments into a practical, enabling framework, allowing people to discuss a light switch, a door, or a telephone not as distant tasks but as controllable elements of a familiar environment. In occupational therapy, ECUs are not merely devices; they are instruments of autonomy that shape a person’s day-to-day possibilities, mood, and sense of place within their own home. Yet, as the literature from the British Journal of Occupational Therapy and related practice shows, access to these meaningful tools remains uneven. Funding policies, service organization, and the capacity to provide ongoing support create a landscape in which the beneficial potential of ECUs can be unevenly distributed. This chapter considers the funding and accessibility dimensions of ECUs within occupational therapy, tracing how policy, practice, and patient advocacy converge to determine who benefits and under what conditions. It also examines how the field might respond to persistent disparities while preserving the core therapeutic aims of ECUs: independence, safety, and social participation in daily life.\n\nThe evolution of ECUs from simple, local actuation to networked, intelligent systems mirrors broader shifts in rehabilitation toward person-centered, technology-enabled care. Historically, ECUs were prized for their capacity to compensate for loss of functional movement in the upper and lower limbs, enabling control over lighting, heating, household appliances, and basic communication devices. In England, as described in contemporary occupational therapy literature, the need for ECUs arises from long-term physical impairments due to disease, trauma, or congenital conditions. The practical benefit is straightforward: a user who cannot manipulate a standard switch, push a door button, or dial a phone can still access the channels of daily life that many people take for granted. However, the path from need to outcomes is mediated by the funding and service infrastructure that supports ECUs, and that mediation is where many people encounter friction.\n\nFrom the outset, the central challenge is cost. ECUs, particularly when they are customized to fit a person’s home and functional profile, demand not only the initial hardware but also bespoke installations, training, and ongoing technical support. In many systems, public health coverage is partial or contingent on strict eligibility criteria. This partial coverage is not merely a question of dollars; it reflects broader priorities and systems-level decisions about who receives what kind of assistive technology and when. For users in lower socioeconomic circumstances or in regions with limited healthcare resources, the likelihood of timely access diminishes, and the consequences extend beyond the device itself. When ECUs are delayed or denied, individuals lose not only a tool but an opportunity to re-engage with daily routines, participate in social life, and maintain a sense of agency that can be hard to reclaim later.\n\nThe 1997 study by SA Holme, published in the British Journal of Occupational Therapy, remains a touchstone for understanding these dynamics. Holme highlighted that ECUs could substantially improve autonomy and quality of life for people with spinal cord injury or other serious motor impairments, yet implementation was hampered by inconsistent funding policies, limited availability of trained professionals to assess needs and install systems, and assessment processes that did not always capture the full range of user requirements. The study underscored a paradox: even when technology exists that can reduce dependence on caregivers and increase independence, system-level barriers can impede access. The implications of that insight extend into contemporary practice as much as they did twenty-five years ago. The persistent challenge is not simply to produce better devices but to ensure that the pathway to obtaining them is fair, transparent, and capable of supporting long-term use.\n\nA contemporary perspective in occupational therapy continues to frame funding as a critical determinant of equitable access to ECUs. The question is not simply whether a device can be prescribed, but whether a user can realistically receive training, installation, and ongoing maintenance within a reasonable timeframe. The reality in many health systems is that funding decisions are shaped by bureaucratic processes, budget constraints, and regional variances in service provision. In some regions, ECUs may be funded through dedicated assistive technology schemes, while in others they are covered only as part of broader rehabilitation packages or not at all. Even when devices are funded, the ongoing costs of maintenance, software updates, sensor recalibration, and eventual replacement pose recurring burdens. These costs are not trivial; they accumulate over time and can outstrip a patient’s or family’s capacity to manage them without additional support.\n\nThe practical outcome of such funding landscapes is a differential access to ECUs that mirrors broader patterns of health inequality. People from higher-income households often have better access to private assessment services, quicker installation timelines, and more robust post-purchase support networks. In contrast, those with fewer financial resources or who live in under-resourced areas may experience long waiting periods, fragmented assessments, or limited access to technicians with the necessary expertise. The consequence is not merely a delay in technology but a widening gap in opportunities for participation in home life, employment, schooling, and community activities. Occupational therapists are frequently the frontline advocates within multidisciplinary teams, translating clinical need into a funding request, outlining home modifications alongside ECU recommendations, and coordinating training and follow-up. Yet even the most diligent OT cannot overcome an arbitrary or opaque funding structure; systemic clarity and consistency are prerequisites for equitable patient outcomes.\n\nIn thinking about policy and practice, it is essential to consider how ECUs intersect with broader shifts in healthcare delivery. The integration of ECUs with mainstream technologies—such as smartphone interfaces, voice assistants, and cloud-connected devices—promises greater flexibility and user-friendliness. This convergence raises important questions about regulatory classifications and reimbursement pathways. ECUs have typically been categorized as medical devices, with many traditional systems falling under Class 1 medical device classifications under EU regulations. As more consumer technologies are incorporated into ECU ecosystems, there is a plausible expectation that regulatory frameworks will evolve to reflect increased functionality, complexity, and integration with digital health ecosystems. For occupational therapists, this evolution carries both promise and risk: promise in expanded capabilities and potential for more seamless home use, and risk in creating more complex maintenance requirements or shifting the burden of cost and upkeep toward patients.\n\nAnother dimension that deserves attention is accessibility beyond physical access to the device itself. Sensory impairments, most notably vision loss, can complicate access to ECUs, and patients with coexisting sensory or cognitive impairments may require additional supports. The current funding and service models, however, have historically prioritized motor impairments. This separation can inadvertently leave individuals who have multiple challenges without a holistic pathway to environmental control. From an OT standpoint, this means adopting a holistic assessment that accounts for sensory, cognitive, and psychosocial factors alongside motor capability. It also means recognizing the need for training that is adaptive and accessible to a wide range of users, including those who may learn through non-traditional means or require ongoing coaching to maintain skill proficiency.\n\nIn practice, the assessment process itself becomes a central hinge upon which equity turns. An optimal OT assessment considers not only the user’s current capabilities and home environment but also the user’s long-term goals, the likelihood of functional progression or stabilization, and the user’s social support network. It should also anticipate the realities of home life, including caregiver availability, travel constraints, and the financial constraints that might affect ongoing use of the ECU. A robust plan will integrate device selection with home adaptation, training for the user and caregivers, and a maintenance schedule. It will also outline contingency strategies for device failure or changes in health status. The sensitivity of such assessments to local resources means that equitable practice often requires OTs to engage in advocacy—not just for the initial purchase, but for the entire lifecycle of the ECU.\n\nAdvocacy is not merely a clinical task; it is a professional and ethical imperative. In this regard, the literature emphasizes that patient needs must be represented within the healthcare system with clarity and persuasiveness. One resource that offers practical examples of advocacy strategies can be useful here: Examples of advocating for patient needs within the healthcare system. By highlighting real-world scenarios where patients secured access to services through coordinated efforts—interdisciplinary teams, social work input, and policy-level engagement—therapists can frame ECU funding not as a luxury but as a necessary component of functional rehabilitation and social participation. The act of advocacy, however, must be grounded in evidence-based practice and transparent criteria. It is not enough to push for access; there must be rigorous documentation of functional need, a clear plan for training and support, and a realistic budget that reflects the ongoing nature of device maintenance and re-evaluation.\n\nA further challenge is ensuring that the knowledge and skills required to implement and support ECUs are distributed across the system. Holme’s early observations about the scarcity of trained personnel still resonate in many settings. The modern OT workforce needs ongoing professional development to stay current with evolving technologies, including eye-tracking interfaces, voice-activated controls, and multi-modal input systems. Training cannot be a one-off event; it must be embedded in service delivery, with opportunities for follow-up, recalibration, and user-driven customization. Moreover, the home environment presents its own demands: electrical wiring standards, furniture arrangement, and potential safety considerations need to be addressed in collaboration with electricians, caregivers, and the user themselves. The complexity of this process reinforces the point that funding alone cannot secure successful ECU outcomes; integrated care pathways and cross-disciplinary collaboration are essential for translating funding into real-world independence.\n\nThe NHS in the United Kingdom, along with other health systems, has moved toward recognizing ECUs as a cornerstone of both physical rehabilitation and social inclusion. Modern practice in many NHS ECU services includes not only device provision but also training for digital literacy, access to online communications, and support for engaging with digital environments. This broader approach aligns with the understanding that environmental control extends beyond the immediate physical space. A person may wish to access online education, maintain social connections through digital platforms, or use assistive technologies to participate in work or volunteering. In this context, ECUs become enablers of digital inclusion as well as physical autonomy. Yet, this expanded scope also places additional demands on funding streams and service capacity. If ECUs are to serve as doors to both the home and the wider digital world, then clinicians must advocate for funding structures that cover not only the initial device but also the necessary software updates, training modules, and access to ongoing technical support that such systems require.\n\nThe experience of funding ECUs is thus a story of balancing immediacy with sustainability. A timely device that arrives after a long wait can transform a person’s daily life, yet without ongoing support, that same device can rapidly lose its value. Sustainability includes not only finance but also the practicalities of maintenance, calibration, and eventual replacement. In regions where the health service is under-resourced, patients may be asked to bear disproportionate costs or to navigate opaque processes that blur the line between medical devices and consumer electronics. The therapeutic relationship, therefore, becomes a critical vehicle for ensuring that the user’s voice is heard within the system. Therapists must document outcomes in ways that matter to funders—quality of life improvements, reductions in caregiver burden, and measurable increases in independence—without losing sight of the user’s lived experience. This requires a narrative of care that complements quantitative metrics with qualitative stories of everyday benefit.\n\nTo date, the literature and practice guidelines continue to call for clearer funding pathways, standardized assessment processes, and robust post-purchase support. The goal is to move toward equitable access that does not depend on a person’s postcode, income, or the presence of a specialized center nearby. Achieving this requires collaboration among occupational therapists, funding bodies, policymakers, manufacturers, and community organizations. It also requires ongoing research that updates the evidence base for ECU effectiveness, cost-effectiveness analyses, and evaluations of long-term outcomes. In particular, there is a need for contemporary studies that examine how ECUs interact with newer digital ecosystems, how maintenance costs evolve over time, and how user training can be optimized to minimize reliance on external support while maximizing user autonomy. The patient journey from referral to independent use is not linear, and every stage presents opportunities to reduce barriers while safeguarding safety and dignity.\n\nIn closing, the question of funding and accessibility for environmental control units is not simply economic or logistical. It is a question of value—what society chooses to invest in as part of its obligation to people with significant disabilities. ECUs have the potential to reshape daily life, but their success depends on the compatibility of clinical judgment, policy design, and practical support. Occupational therapists stand at the center of this ecosystem, translating need into a plan, guiding families through complex processes, and ensuring that the therapeutic benefits of ECUs are realized in durable, meaningful ways. If the field can advance toward transparent funding criteria, scalable training models, and integrated care pathways, ECUs will more reliably deliver on their promise: to open doors, enable independence, and reduce the invisible weight of daily tasks that many take for granted. For readers seeking historical context and clinical implications of ECU use, the foundational work in the field provides a compass for future practice and policy work alike: https://journals.sagepub.com/doi/abs/10.1177/030802269706001005
Final thoughts
Environmental Control Units are invaluable assets in occupational therapy, aiding individuals with physical impairments in gaining control over their environment and enhancing their independence. By understanding ECUs, recognizing the vital role of occupational therapists, leveraging technological advancements, and addressing funding issues, we pave the way for more inclusive solutions in rehabilitation. As businesses and stakeholders, supporting these initiatives not only enhances the quality of life for users but also aligns with the growing demand for accessible technology in healthcare. Sustainable investment in ECUs represents more than just a medical necessity; it is a commitment to fostering independence and dignity for individuals facing physical challenges.