Physical occupational therapists play a critical role in enhancing mobility, reducing pain, and restoring function for individuals recovering from injury or illness. As their services become more integral to rehabilitation, business owners in the healthcare sector need a comprehensive understanding of their contributions. This article explores the multifaceted role these therapists play within rehabilitation settings, outlines the educational and licensing requirements essential for their practice, and highlights the collaborative efforts they engage in with other healthcare professionals to ensure optimal patient outcomes. Each chapter builds upon this understanding to paint a holistic view of the profession’s value in modern healthcare.
Reclaiming Movement and Independence: The Integrated Role of Physical and Occupational Therapists in Rehabilitation
Rehabilitation is rarely a straight line from injury to independence. It unfolds as a dialogue between bodies, environments, and the people who guide them. In this conversation, physical therapists and occupational therapists act as complementary conductors, each carrying a distinct yet overlapping repertoire of skills designed to restore not only movement but also meaningful participation in daily life. The aim is not merely to return someone to a baseline of function but to harmonize strength, balance, and dexterity with the capacity to manage real-world tasks in real homes, workplaces, and communities. When this alignment occurs, patients don’t just move again; they re-enter their life with confidence, purpose, and an increased sense of autonomy that governs every choice from dressing to driving, from preparing a meal to replying to a child’s call for help. The chapter that follows traces this integrated role, showing how physical and occupational therapy—together and with others on the care team—shape rehabilitation as a holistic, person-centered enterprise rather than a sequence of isolated interventions.
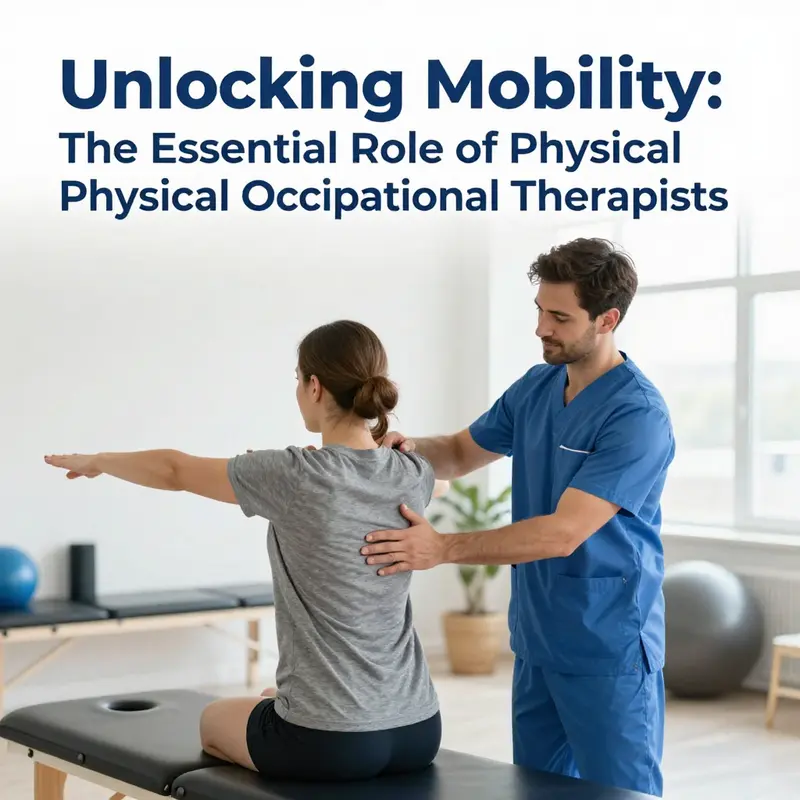
In clinical settings, physical therapists (PTs) and occupational therapists (OTs) begin with a shared commitment to restoring functional movement and independence, yet they arrive with different lenses. PTs focus on the mechanics of movement—how joints flex and extend, how muscles generate force, how the nervous system coordinates a sequence of steps. They guide patients through therapeutic exercises that build strength, improve range of motion, and enhance balance and endurance. Manual therapy, precise palpation, and the judicious use of modalities such as heat, cold, ultrasound, or electrical stimulation provide the physical framework for recovery. But motion is not merely a mechanical event; it sits within a lived daily routine. This is where occupational therapists bring their perspective. OTs examine the tasks that give life meaning—adapting the environment, selecting assistive devices, and teaching strategies that compensate for limitations while maximizing engagement in important roles. Dressing, bathing, cooking, managing finances, returning to work, and participating in social activities are not afterthoughts; they are the coordinates by which health is measured in the real world.
The partnership between PTs and OTs rests on a shared method: assess, plan, implement, and adapt in the service of a person’s goals. Assessment in rehabilitation blends objective measurement with patient-reported experience. A PT might quantify gait speed, leg strength, or the symmetry of a step, while an OT observes how those same improvements translate into the ability to tie a shoe, button a shirt, or prepare a simple meal. This is not a competition of numbers but an alignment of data with daily purpose. The plan then becomes a living document, one that evolves as the patient learns to apply improved movement to tasks that matter most. Goals are not abstract targets; they are statements of participation—for example, “I want to walk to the mailbox without assistance” or “I want to return to volunteering at the community center.” When therapists share a goal-centered frame, they create a trajectory that integrates musculoskeletal recovery with practical competence, a trajectory that honors the patient’s values and life story.
The day-to-day work of rehabilitation unfolds in a spectrum of settings—from hospital wards where acute stabilization gives way to safer movement, to outpatient clinics where complex gait or hand function retraining takes place, to in-home programs that emphasize carryover into daily life. In each environment, PTs and OTs adapt their practices to the rhythm and constraints of the setting, always guided by the same principle: a patient’s progress is measured not by how many repetitions were completed in a session but by how well the patient can continue that progress outside the clinic, in the patient’s own space and schedule. This continuity is achieved through careful education and the development of sustainable home programs. A PT may outline a progressive exercise routine to strengthen the hip and trunk that supports safe transfers, while an OT translates that improvement into a practical sequence, such as how to reach a kitchen counter safely or how to navigate a bathroom with fewer slips and more stability. The synergy is practical and intimate, a daily choreography of strengthening, task analysis, environmental modification, and patient embodiment.
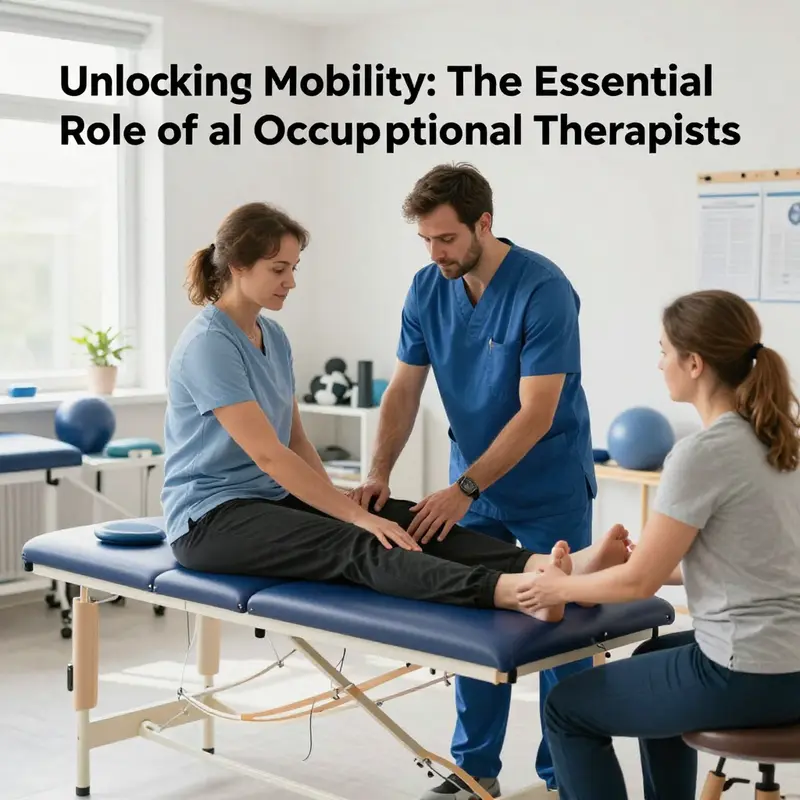
Consider the experience of a patient recovering from a stroke. The PT guides neuro-rehabilitation through targeted movements: promoting weight bearing through the affected limb, encouraging a symmetrical gait, and re-establishing motor patterns that restore walking efficiency. The OT, meanwhile, analyzes the moment-to-moment demands of home life. They examine how the patient can remove liquids from the fridge, use adaptive tools to reach high shelves, or reorganize a kitchen to reduce the risk of spills. They also address cognitive aspects that influence safety and independence, such as sequencing tasks, planning multi-step activities, and managing memory challenges that accompany brain injury. Together, they translate neural recovery into practical competence. The PT provides the strength and control needed for forward movement; the OT ensures that forward movement translates into an unencumbered ability to perform essential life tasks. The patient’s return to routine—taking a shower without fear of slipping, cooking a simple meal, or dressing without assistance—becomes the measure of success, a proof that rehabilitation has moved from protocol to possibility.
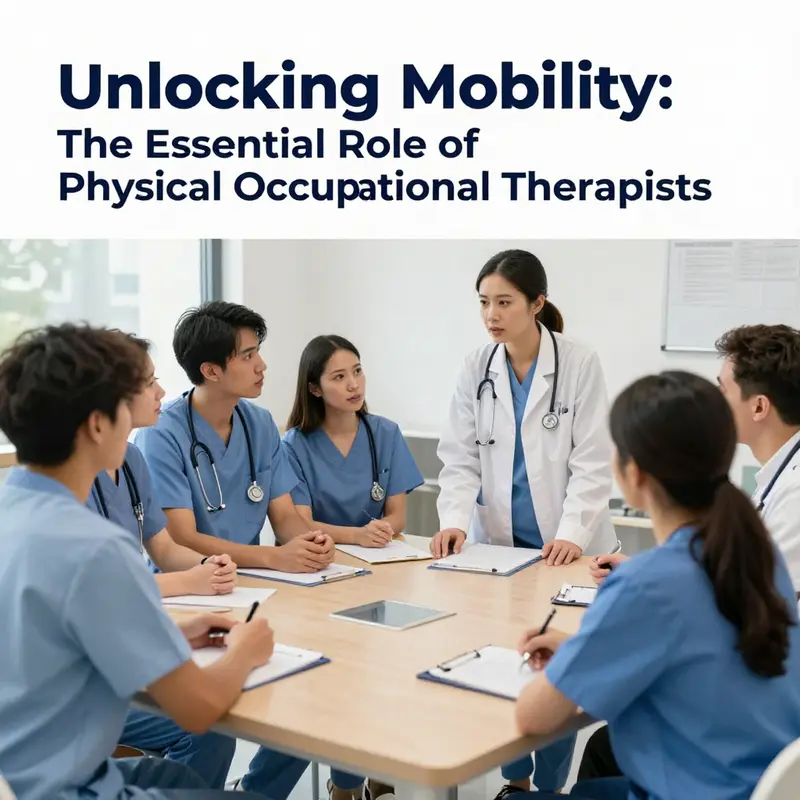
A crucial facet of this integrated approach is collaboration. Interprofessional teamwork enables therapists to tailor interventions to the patient’s evolving needs and to anticipate barriers before they arise. Close communication with physicians ensures medical stability and clear care plans, while nurses contribute ongoing monitoring and support. Psychologists or mental health professionals may become involved when motivation, mood, or cognitive changes complicate rehabilitation, ensuring the patient’s emotional framework aligns with physical and functional goals. Such collaboration is not a matter of adding voices; it is about creating a coherent narrative in which each professional’s expertise informs a unified strategy. The most effective rehabilitation emerges when physical and occupational therapies are not siloed chapters but interwoven threads of a single story, told through a common language of function, safety, and participation. In practice, this means joint goal setting, shared progress notes, and synchronized discharge plans that ensure patients remain supported as they transition from clinical care to home-based practice and community engagement. The result is a rehabilitation experience that respects the person’s history, acknowledges the real-life contexts in which movement occurs, and uses evidence-based practice to optimize outcomes.
Education lies at the heart of empowering patients to sustain gains once they leave the clinic. Education includes how to perform exercises safely, how to manage pain without escalating reliance on medications, how to recognize warning signs that require medical attention, and how to modify daily routines to prevent relapse or compensatory injuries. PTs and OTs each contribute a strain of knowledge that reinforces the other. The PT helps patients understand the mechanics of movement, the limits of strength, and the wiser pacing of activity. The OT translates those mechanics into a repertoire of practical skills—how to adapt furniture, how to use assistive devices properly, and how to modify the environment to reduce cognitive load during daily tasks. When patients understand not just what to do but why it matters in the context of their daily lives, adherence improves, and long-term outcomes improve as well. This educational cornerstone extends beyond instruction; it fosters resilience. Patients learn to self-monitor, adjust, and anticipate new challenges, which reduces the likelihood of relapse and promotes a smoother re-entry into the routines that define their sense of normal.
The breadth of rehabilitation work extends across populations and settings. In hospitals, PTs and OTs often begin with acute stabilization, ensuring patients can safely mobilize and participate in essential care activities. In outpatient clinics or community-based programs, their focus shifts toward restoration of function, return to driving or work, and re-engagement with social roles. Home health visits bring therapy into the living space, addressing real-world obstacles and enabling caregivers to support the patient’s progress. The elderly, for whom fall prevention becomes a central theme, see therapists working on balance, gait optimization, fine motor control, and the environmental modifications that minimize risk. Pediatric populations benefit from play-informed activities and activity analysis that integrates movement with school participation and family routines. Each case demands a bespoke blend of PT and OT expertise, not only to improve physical capacity but to nurture the confidence and autonomy that define a meaningful life. In all cases, the overarching objective remains consistent: to reduce pain where it limits action, to restore safe and efficient movement, and to enable participation in the activities that confer purpose and identity.
Despite the clinical precision that informs practice, rehabilitation remains deeply human. The therapist’s role goes beyond technique; it involves listening to a patient’s story, values, and goals. A person might describe a desire to care for grandchildren with unassisted independence, to return to a professional role, or to resume a cherished hobby. Therapists translate these aspirations into measurable steps and meaningful milestones. They validate fear and frustration while encouraging incremental victories, recognizing that rehabilitation is often non-linear, punctuated by plateaus and breakthroughs. In this way, PTs and OTs help patients not only recover function but also rebuild a sense of agency. The partnership becomes a vehicle for restoring dignity as people relearn their bodies and relearn what their bodies can do in the context of the lives they want to lead.
Professional preparation supports this work. The field requires a Doctor of Physical Therapy degree for practice in the United States, followed by licensure in each state and successful completion of a national examination. The path reflects the seriousness with which the profession treats safety, efficacy, and ethical practice. The American Physical Therapy Association (APTA) and the American Academy of Physical Medicine and Rehabilitation (AAPMR) provide guidance, standards, and ongoing education that help therapists stay current with evolving evidence and clinical techniques. While the focus in this chapter centers on integrated rehabilitation, the broader landscape of professional development is a reminder that knowledge is dynamic, and the best therapists continually refine their approaches in light of new research, patient feedback, and changing health care environments. When PTs and OTs commit to lifelong learning, they remain capable of meeting the complex demands of diverse patients and advancing the boundaries of what rehabilitation can achieve.
In the end, the synergy between physical and occupational therapy is not merely an academic distinction but a practical philosophy. It embodies a holistic understanding that movement and daily life are inseparable facets of well-being. Movement without context risks becoming a hollow achievement; daily life without movement risks becoming impossible. The integrated model honors both sides of the coin, aligning the body’s capacity with the tasks that give life meaning. This unity resonates across all ages and conditions, from stroke recovery to arthritis management, from spinal cord injuries to post-surgical rehabilitation, and from cognitive challenges to the emotional dimensions of disability. Through shared goals, collaborative practice, and a patient-centered ethic, physical and occupational therapists orchestrate a rehabilitation journey that is as much about rediscovering purpose as it is about restoring function. The patient who learns to tie a shoelace, prepare a simple meal, and stand with confidence at the bathroom sink embodies the essence of this collaboration: a life regained not by a single intervention, but by a coordinated, compassionate, and scientifically grounded partnership.
For readers seeking a deeper dive into the practical and collaborative dimensions of this work, consider exploring additional perspectives on how therapists coordinate care with other professionals and how that collaboration translates into better patient outcomes. How occupational therapists collaborate with other healthcare professionals offers a concise exploration of teamwork dynamics that underscore the themes described here. This broader lens helps frame rehabilitation as a system in which each professional contributes a piece of the whole, ensuring that interventions are coherent, patient-centered, and sustainable as individuals move through the recovery journey. As the field continues to evolve, the core message remains clear: movement and life are best supported when therapists work in concert with patients, families, and the wider health care team, guided by evidence, empathy, and an unwavering commitment to function-centered care.
External resources for further reading on professional guidelines and standards can be found through the broader clinical community, including organizations that shape best practices in rehabilitation. See https://www.aapmr.org/ for additional context on the role of rehabilitation specialists and their evolving contributions to the care of individuals with movement disorders and functional impairments.
Pathways to Practice: Education, Registration, and the Dual Role of Physical and Occupational Therapy
Education and Licensure for Practitioners Bridging Physical and Occupational Care
Becoming a clinician who operates at the intersection of physical rehabilitation and functional occupation requires more than technical skill; it requires a deliberate educational path and formal licensure that verify competence, safeguard patients, and enable collaboration across care teams. Whether you identify primarily as a physical therapist or an occupational therapist, the educational frameworks and registration processes shape the day-to-day scope of practice, influence how you assess and treat patients, and determine the settings in which you can work. This chapter explains the typical academic progression, the regulatory milestones that lead to registration, and the practical implications of meeting these standards—particularly in an Australian context where distinct but complementary routes exist for physical and occupational professionals.
At the foundation of either pathway lies a rigorous university program. For physical therapy, modern professional qualifications have moved toward entry-level master’s or doctoral standards. In Australia, accredited postgraduate programs such as the Master of Physiotherapy or Doctor of Physiotherapy provide the theoretical knowledge and clinical reasoning frameworks modern practice demands. These programs blend anatomy, biomechanics, neuroscience, and pathology with applied clinical modules that emphasize assessment, manual therapy, therapeutic exercise, and evidence-based practice. Occupational therapy education follows a parallel structure: accredited Bachelor or Master of Occupational Therapy programs teach human development, activity analysis, environmental adaptations, and approaches to promoting independence in daily living. Both curricula include supervised clinical placements where students apply classroom learning in real-world settings, refine hands-on skills, and learn professional communication.
Clinical placements are pivotal. They expose students to diverse populations—orthopaedic, neurological, paediatric, geriatric, and mental health cases—so candidates gain experience across the lifespan. Placements also build interprofessional skills; learners collaborate with doctors, nurses, speech pathologists, social workers, and allied health colleagues. Students learn to prioritize patient goals, navigate risk, and adapt interventions to the environment. These supervised encounters are where theoretical models meet messy clinical reality, where a plan of care is adjusted because of a home hazard, cognitive limitation, or lack of social supports. Such adaptations highlight why both professions emphasize not just technical interventions but also patient education, goal setting, and collaborative problem solving.
Accreditation matters because it determines eligibility for registration. In Australia, professional programs must meet standards set by the relevant accrediting and regulatory bodies. For physiotherapists, the Australian Physiotherapy Council oversees accreditation and ensures programs produce graduates who meet current competency expectations. For occupational therapists, the Occupational Therapy Board of Australia (operating under the Australian Health Practitioner Regulation Agency, AHPRA) verifies program quality and outcomes. Completing an accredited degree is the first checkpoint toward safe, ethical practice and legal registration.
Registration transforms academic qualification into legal permission to practise. In Australia, AHPRA administers registration across health professions, requiring applicants to meet academic, language, and character standards. For local graduates, the pathway tends to be straightforward: graduate from an accredited program, demonstrate English proficiency if needed, and satisfy background checks. Internationally qualified applicants follow additional steps designed to confirm equivalence of training and safe practice readiness. For physical therapists who trained overseas, the Physiotherapy Competency Assessment Program (PCAP) evaluates knowledge and skills against Australian standards. Occupational therapy applicants may undergo a two-stage assessment: a desktop review of qualifications and experience, followed by a Supervised Practice Assessment (SPA) that typically involves a specified number of supervised practice hours under a registered occupational therapist. These measures are not bureaucratic hurdles alone; they are quality safeguards that protect patients and ensure practitioners can meet local clinical expectations.
English language competence and criminal history checks are common elements of registration. Health care involves complex communication with patients and colleagues; proficiency in language is essential for assessment, informed consent, and safety. Similarly, background screening verifies that practitioners meet standards of good character, a requirement intrinsic to public trust in health services. Meeting these criteria finalizes the transition from student to registered clinician and opens employment opportunities across hospitals, community services, private clinics, residential aged care, and home-based care.
Licensure also defines the legal scope of practice. Registered physiotherapists are authorized to assess, diagnose movement-related conditions, and deliver interventions aimed at restoring mobility and function. Registered occupational therapists are authorised to evaluate functional performance in daily activities and to recommend and implement interventions that increase independence and participation. Understanding the distinctions is crucial for professionals who work at the border of the two disciplines. A clinician trained and registered as a physiotherapist should remain within the physiotherapy scope unless they hold occupational therapy qualifications and registration. Likewise, occupational therapists should avoid practising physiotherapy beyond their credentialing. This separation protects patients: each profession has unique competencies, clinical frameworks, and evidence bases that guide practice.
Yet, the reality of clinical care often requires blended competencies. Rehabilitation is patient-centered and goal-driven, and many goals require overlapping skills. A stroke survivor, for example, may need a physiotherapist to address balance and gait retraining and an occupational therapist to relearn dressing, cooking, or returning to work. In multidisciplinary teams, professionals complement each other—each applying their specialized lens to the patient’s problems. For those who wish to develop hybrid expertise, dual qualifications are an option. Some clinicians pursue additional postgraduate training in allied disciplines or obtain both occupational therapy and physiotherapy credentials. While this represents a considerable investment in time and study, it produces clinicians with a versatile clinical toolkit and a capacity to integrate mobility promotion with functional adaptation seamlessly.
Postgraduate education and continuing professional development (CPD) are another dimension of professional growth. After initial registration, clinicians must keep their knowledge current, maintain skills, and reflect on practice. CPD activities include formal courses, workshops, clinical supervision, research participation, and self-directed learning. Regulatory boards often require evidence of CPD for annual registration renewals. Beyond compliance, CPD fuels clinical excellence. It enables practitioners to adopt new evidence-based techniques, refine assessment accuracy, and expand their capacity to manage complex cases. For example, learning advanced manual therapy or neurological rehabilitation approaches can change outcomes in patients with chronic pain or traumatic brain injury. Similarly, occupational therapists may pursue specialized training in sensory integration, cognitive rehabilitation, or assistive technology to broaden their intervention options.
Supervised practice for international graduates deserves emphasis because it bridges differences in training models. The supervised practice period allows international clinicians to adapt to local clinical norms, documentation standards, and interdisciplinary workflows. It also provides employers with confidence that the clinician can perform safely in their context. Supervised practice is not merely oversight; it is a structured learning phase where mentors guide clinical reasoning, ethical decision-making, and communication skills. For domestic graduates, early career mentorship and structured a junior clinician program can serve a similar function, smoothing the transition into independent practice.
Regulatory landscapes evolve, and practitioners must be aware of current requirements. In Australia, AHPRA provides authoritative details on registration, scope of practice, and accreditation standards. Policy changes—such as adjustments to English language thresholds, competency assessment processes, or CPD expectations—can affect both new applicants and established practitioners. Staying informed is a professional responsibility; it ensures compliance and the continuous delivery of safe, effective care.
Education and licensure also shape career mobility. Registered clinicians can practice across a range of settings and move between public and private sectors. They may also transition into roles in education, research, policy, and management. Some pursue a clinical specialisation recognised by peak bodies, while others follow a generalist career that values breadth. Employers often seek evidence of registration, relevant postgraduate credentials, and CPD engagement when hiring. For those interested in international practice, understanding comparable registration processes in target countries is crucial. Reciprocal recognition arrangements are limited; many countries require their own assessment of competence.
Finally, ethics and professionalism are woven into education and registration. From the first day of university to ongoing practice, clinicians are expected to uphold patient-centred care, informed consent, confidentiality, and cultural competence. Registration boards enforce standards of professional conduct and investigate complaints. Maintaining registration involves not only technical competence but also adherence to ethical responsibilities. This holistic view of practice ensures that competency encompasses both skill and character.
For clinicians and students navigating training choices, the key is alignment between career goals and credentialing pathways. Choose an accredited program that prepares you for registration. Seek placements that broaden clinical exposure. Plan for supervised practice or competency assessments if you trained overseas. Commit to lifelong learning to keep pace with evolving evidence. And, if your goal is to integrate physical and occupational perspectives, consider dual qualifications or deliberate postgraduate study that builds complementary skills. These choices shape not only your scope of practice but also your ability to collaborate effectively in multidisciplinary teams and to deliver care that restores movement and meaningful participation in life.
For official, current details on physiotherapist registration requirements in Australia, consult the AHPRA registration portal: https://www.ahpra.gov.au/Registration/Find-a-Health-Professional.aspx?profession=physiotherapist
For more on how occupational therapy and physical therapy compare in goals and approaches, see this discussion of occupational therapy vs physical therapy that examines roles and distinctions in practice: occupational therapy vs physical therapy.
Bridging Movement and Meaning: The Collaborative Practice of Physical and Occupational Therapists in Healthcare
In the tapestry of modern rehabilitation, the collaboration between physical therapists and occupational therapists stands as a core thread that binds movement to daily meaning. When patients leave a hospital bed or a therapy clinic with greater range of motion or stronger muscles but still struggle to bathe, dress, or prepare meals, the true victory lies in translating physical gains into functional independence. This is where collaboration becomes more than a courteous handshake between professionals; it is the deliberate alignment of two distinct yet complementary expertise, woven together to support a person’s capacity to participate in life as they choose it. The physical therapist’s lens focuses on mobility, stability, strength, and the nervous system’s response to movement. The occupational therapist’s lens centers on the person’s performance in everyday activities—feeding, dressing, housekeeping, work tasks, and social roles—within the context of the person’s environment and values. When these perspectives converge in a coordinated plan, outcomes extend beyond lab-based measures of strength or range of motion to the meaningful improvements in daily living that matter to patients and families alike. This integrated approach is not incidental; it reflects a shift toward patient-centered care in which teams share goals, synchronize interventions, and align documentation to reflect a single, coherent pathway toward recovery and adaptation.
The clinical reality of collaborative practice begins with shared assessment and a joint recognition that each therapist brings a unique, indispensable piece to the rehabilitation puzzle. In practice, a patient recovering from a stroke or joint replacement moves through a continuum of care in which both therapists contribute, often in the same session, to a composite treatment plan. The physical therapist might guide the patient through task-specific strengthening, gait training, or neuromuscular re-education, while the occupational therapist tunes the patient’s capacity to sit, reach, and manipulate objects during daily routines. Yet the most important insight comes when the team looks at the patient holistically—how a stronger knee or improved trunk control translates into safer transfers, how increased dexterity supports kitchen tasks, and how the ability to plan and sequence steps affects a patient’s confidence to return to a job or a cherished hobby. In this framework, collaboration becomes a mechanism for accelerating progress and for ensuring that progress is functional rather than purely physiological.
The synergy between physical and occupational therapy is especially evident in rehabilitation settings where joint treatment is not merely convenient but essential. Consider a patient in post-surgical recovery who is rebuilding strength and flexibility after a complex knee procedure. The physical therapist may emphasize correct alignment, controlled loading, and progressive resistance to restore stability and endurance. The occupational therapist concurrently assesses how these gains translate into safe, independent daily activities, such as navigating the kitchen, managing personal care, and planning a simple morning routine that preserves energy for the day ahead. The two disciplines intersect when the plan shows that improved knee function must yield improved independence with toileting routines, dressing, and meal preparation. This integration ensures that improvements in movement do not occur in a vacuum but are applied in the real world where choices about work, social participation, and family roles are made.
Effective collaboration rests on several shared mechanisms that enable teams to move beyond mere coexistence toward coordinated action. At its core is a model of shared goal setting, where the patient, family, and all members of the rehabilitation team contribute to a common destination. Rather than two therapists pursuing parallel objectives, they craft a unified roadmap with measurable milestones that reflect both mobility and activity performance. Regular communication becomes the glue that keeps the plan coherent across sessions, shifts in patient status, and changes in goals as recovery unfolds. Documentation, too, moves from fragmented notes to a unified narrative that describes not only what was done, but how the patient’s performance in daily tasks evolved in parallel with improvements in physical capacity. In many settings, these practices draw on established teamwork frameworks that emphasize transparency, mutual respect, and role clarity, ensuring that each professional’s contributions are valued and integrated rather than competing for primacy.
The practical expressions of collaboration often emerge as co-treatment sessions, where therapists work side by side to address overlapping goals. In a stroke rehabilitation scenario, a patient might perform a coordinated activity that requires both movement and functional execution: transferring from bed to chair, then applying a dressing or buttoning a shirt while maintaining balance. The physical therapist might monitor gait safety and leg strength while the occupational therapist guides the patient through sequencing and motor planning required to complete the task smoothly. This co-treatment approach reduces the number of transitions the patient must make between appointments and reinforces the real-world relevance of rehabilitation. It also creates opportunities for immediate problem-solving and reassurance, as caregivers observe therapists modeling how mobility improvements translate into independence. The patient witnesses a visible link between what seems like abstract therapeutic concepts—muscle activation, proprioception, motor planning—and a concrete outcome—being able to dress without assistance.
From a systems perspective, the consolidation of physical and occupational therapy in patient care benefits from structured collaboration models that foster consistency and scalability. The Collaborative Planning (CP) model, initially developed to support nursing and occupational therapy partnerships, offers principles that are broadly applicable to PT-OT teams: clearly defined shared goals, regular and purposeful communication, and unified documentation that captures a patient’s progress across domains. When adapted thoughtfully, these principles help physical and occupational therapists synchronize their assessment tools, align treatment timelines, and coordinate discharge planning. The result is not just a smoother workflow but a more precise calibration of interventions to patient outcomes. In effect, the model reframes collaboration as a deliberate design choice rather than an incidental byproduct of working in the same space.
A broader context for this partnership appears in the integration of occupational therapists into primary health care settings. Across many health systems, primary care acts as the arena where early intervention, prevention, and the management of chronic conditions unfold. In such environments, physical and occupational therapy teams must harmonize their approaches to address conditions like arthritis, fall risk, or cognitive-communication challenges that impede participation in daily life. The emphasis shifts toward prevention, education, and environmental modification, with therapy teams supporting patients in maintaining function and independence outside hospital walls. In primary care, OTs bring expertise in activity analysis and environmental adaptation, while PTs contribute strategies to preserve or restore movement and endurance necessary for everyday tasks. Together, they help patients maintain activity levels, minimize disability, and sustain engagement in work, family life, and social roles.
The patient’s perspective sits at the heart of these collaborative endeavors. When the team communicates openly about goals and expectations, patients become active partners in their own care. They gain a sense of control as they observe how improvements in strength and flexibility directly translate into safer and more efficient performance of daily activities. Family members or caregivers are pulled into the dialogue as well, receiving guidance on home safety, adaptive strategies, and the pacing of rehabilitation. In this sense, collaboration becomes patient-centered not only in what is treated but in how care is delivered. It becomes a shared journey in which knowledge from movement science and occupation-based practice converges to empower people to live with less pain, more independence, and a renewed sense of purpose.
The literature on collaboration in occupational therapy provides a valuable lens for understanding how these interdisciplinary efforts translate into better patient outcomes. A core finding is that interprofessional practice improves not only functional gains but also patient satisfaction and satisfaction with care, while reducing hospital stays and readmission rates in certain contexts. In addition, when the care team embeds the principles of collaboration—shared goals, frequent communication, and unified documentation—patients experience smoother transitions between care settings, fewer duplications of testing, and a clearer understanding of what to expect as they move along the recovery trajectory. A robust interprofessional culture can also facilitate innovation, as clinicians draw on diverse expertise to tailor approaches to each patient’s unique life circumstances, preferences, and environments. The concept of collaboration in this context extends beyond the clinical encounter; it shapes the way teams learn from one another, update practices, and foster continuous improvement in patient care.
To operationalize collaboration in daily practice, teams can draw on practical strategies that respect the distinctive identities of physical and occupational therapy while honoring the shared objective of patient participation. First, establish a common language of care. Agree on terminology for goals, progress metrics, and daily activities that matter to patients. Second, synchronize scheduling and session structure to maximize joint opportunities without overburdening patients or staff. Third, deploy cross-training where feasible—allow therapists to observe or learn basic techniques from the other discipline to foster empathy and mutual understanding, while preserving professional boundaries and competence. Fourth, advocate for environmental and systemic supports such as integrated electronic health records and standardized assessment tools that enable seamless information sharing. Fifth, cultivate reflective practice within teams—periodic debriefings after sessions to assess what worked, what did not, and how the plan might be refined to better align movement with daily life. These steps may require cultural change within organizations, but their payoff is a more coherent patient experience, clearer expectations, and a more resilient rehabilitation team.
In reflecting on the trajectory of physical and occupational therapy collaboration, it becomes clear that the future of rehabilitation depends on more than accumulating individual skills. It depends on the capacity of teams to synthesize mobility and activity into a meaningful life for patients. This requires early and ongoing collaboration with education and professional development that teaches interdisciplinary communication, shared decision-making, and joint problem-solving. It also calls for leadership that values integration, supports shared governance, and creates career pathways that encourage therapists to pursue dual competencies or formalized collaborative roles. When such conditions exist, the synergy between movement-based and occupation-based therapies grows from a theoretical ideal into a reliable, everyday practice that shapes how patients regain independence and how healthcare systems deliver care that respects persons as whole beings with histories, goals, and communities.
This chapter has traced the practical and theoretical terrain of collaborative practice between physical and occupational therapists. It has shown how joint assessment, co-treatment, and unified planning translate clinical gains into real-world function. It has underscored how structured collaboration models, when adapted to PT-OT teams, can improve patient outcomes and satisfaction while supporting more efficient care. It has highlighted the role of primary health care as a setting where early intervention and long-term wellness are anchored in interdisciplinary teamwork. And it has acknowledged the barriers that can hinder collaboration—time constraints, documentation fragmentation, and professional silos—while offering concrete strategies to overcome them through shared goals, timely communication, and systemic supports. In short, the alliance between movement and occupation is not just a clinical necessity; it is a moral and practical commitment to helping people live better with less pain, greater independence, and renewed opportunity.
For readers who wish to explore the conceptual foundations of collaboration in greater depth, the field offers rigorous analyses that illuminate how interprofessional practice enhances patient outcomes and team function. A recommended resource is The Conceptual Analysis of Collaboration in the Occupational Therapy Context, which provides peer-reviewed perspectives on how collaboration shapes practice, informs interprofessional relationships, and influences care delivery across settings. This complements the clinical narratives here by grounding everyday teamwork in research-informed principles that advance patient-centered rehabilitation. (MDPI: https://www.mdpi.com/1660-4587/23/1/10)
For further practical reflections on teamwork and collaboration in therapy, readers may refer to how occupational therapists collaborate with other healthcare professionals. This resource discusses the dynamics of interprofessional collaboration in contemporary care and offers concrete considerations for practical implementation. (https://coffee-beans.coffee/blog/how-do-occupational-therapists-collaborate-with-other-healthcare-professionals/)
Final thoughts
Physical occupational therapists are vital partners in the healthcare ecosystem, providing essential rehabilitation services that enhance patients’ quality of life. As we have explored, their roles are not just limited to direct patient care; they are educators, collaborators, and advocates for mobility and health restoration. This comprehensive understanding is necessary for business owners in the healthcare sector to appreciate the full impact of physical occupational therapists within interprofessional teams, thereby fostering a culture of collaboration and patient-centered care.