In the evolving landscape of healthcare, the integration of Occupational Therapy (OT) and Physical Therapy (PT) stands as a vital approach to rehabilitation. These two complementary fields not only aim to restore physical movement and function but also focus on enhancing the overall quality of life for patients. By understanding the foundations and definitions of OT and PT therapy, the various treatment techniques and their applications, the significance of interdisciplinary collaboration, and the future innovations in these therapies, business owners in the healthcare sector can better appreciate their value and implement effective strategies that align with patients’ needs. The following chapters will delve into each of these aspects, providing a holistic overview of how OT and PT therapy can contribute to improved patient outcomes and successful business practices.
From Daily Tasks to Lasting Independence: Foundational Concepts in OT and PT for Holistic Rehabilitation
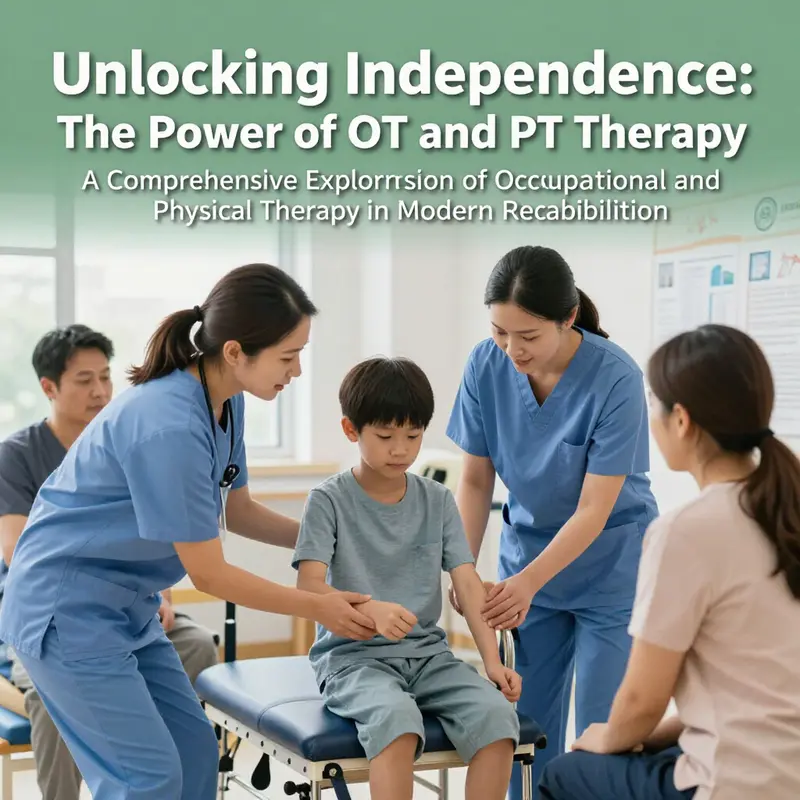
Rehabilitation stands at the intersection of necessity and possibility. When a person invites recovery after an illness, injury, or lifelong condition, the path is rarely about a single remedy or a single moment of relief. It is about a sustained partnership between the body and the environment, a partnership that OT (occupational therapy) and PT (physical therapy) nurture in complementary, deeply human ways. Together they translate medical improvement into practical, meaningful lives. In this chapter, we move beyond the labels of disciplines to examine how OT and PT anchor modern rehabilitation in a shared conviction: recovery is not only about moving pain or regaining strength but about reclaiming the capacity to engage in the activities that define a person’s identity, purpose, and daily rhythm. This is the core of what makes rehabilitation a lived process rather than a series of isolated interventions.
Occupational therapy begins with the understanding that health is inseparable from participation in meaningful life occupations. The word occupation here does not imply a job alone but the full spectrum of activities that structure human life — self-care, domestic responsibilities, work tasks, school-related activities, and leisure. OT prioritizes the client’s goals within their unique environment. It asks not what a person cannot do, but what they want and need to do, and then designs interventions that make those tasks possible again. The therapeutic use of everyday life occupations is the guiding principle, and it rests on a conviction about human health as an adaptive, environmental, and transactional phenomenon. The World Federation of Occupational Therapists articulates this stance plainly: the goal is to enable participation through the therapeutic use of daily life occupations with persons, groups, or populations. This is more than a technique; it is a philosophy of engagement that places the person at the center of care and treats daily life as a site of healing.
The theoretical backbone of OT emphasizes internal and relational processes as much as external skills. Motivation, cognition, emotional regulation, and the person’s relationship to their surroundings shape how they interact with the world and, consequently, how they recover. A patient who has suffered a stroke may regain motor capacity, but OT helps them translate that capacity into practical gains — tying recovery to the ability to dress, prepare a meal, or manage medications. Cognitive and perceptual rehabilitation is often integrated with hand function and dexterity training because daily tasks depend on multiple domains working in concert. The interventions—ADL (activities of daily living) training, hand function work, cognitive exercises, and perceptual retraining—are not isolated drills but purposeful activities that simulate real-life demands. In this sense, OT harmonizes the mind, body, and environment to restore a sense of agency.
Environment is not a backdrop in OT; it is a primary instrument. An OT practitioner will look at a home, a workplace, a classroom, and a community setting and identify barriers to participation. The changes may be as simple as reorganizing the kitchen, installing grab bars, adjusting lighting, or planning safer stair navigation. They may also involve broader considerations, such as selecting and training in adaptive equipment, or advocating for environmental modifications that reduce risk and support independence. The use of assistive technology and adaptive devices is a hallmark of OT practice, enabling people to perform tasks they previously found impossible or unsafe. Even creative and expressive therapies—arts, crafts, music, and games—can be woven into rehabilitation to address emotional well-being, social connection, and a sense of purpose. OT thus treats recovery as a multifaceted journey where physical restoration and life participation reinforce one another.
Physical therapy, by contrast, centers on mobility, movement quality, and physical function. It is especially concerned with restoring biomechanical efficiency, reducing pain, and rebuilding strength, endurance, balance, and coordination. PT is often the frontline response to musculoskeletal injuries, neurological impairments, and post-surgical recovery. The interventions are grounded in physiology, motor control, and biomechanics, yet they are not merely mechanistic. PT practitioners tailor exercise programs, manual therapies, and modalities to each person’s pathology, pain patterns, and functional goals. They guide patients through progressive loading, task-specific training, and gait re-education, aiming to restore confident movement that supports independence in everyday life. In many cases, PT makes possible the initial steps toward more complex tasks and longer-term goals, such as walking longer distances, returning to a sport, or resuming a work-related procedure. The essence of PT lies in reestablishing safe, efficient, and empowered movement, often serving as the physical foundation that allows OT to pursue broader participation.
The dialogue between OT and PT is not a sequence but a symphony. In a typical rehabilitation trajectory, PT may work to restore limb strength and lower the barrier of pain, creating a platform from which a patient can more reliably perform tasks. OT then translates those gains into practical competence: teaching the patient how to don clothing independently, manage personal care, prepare meals, or resume a workplace role in a way that respects both the new motor realities and the realities of daily life. Consider the example of a stroke survivor who regains leg strength through PT and then learns via OT to navigate the home safely, adapt a kitchen for independence, and reestablish social routines that support emotional resilience. In pediatric settings, PT might focus on gross motor skills and postural control, while OT supports fine motor development and school participation, addressing handwriting, tool use, and classroom accessibility. In the domain of sports medicine, PT can restore shoulder mobility after injury, and OT can facilitate a safe return to sport through task-specific, sport-relevant activities that connect the body’s restored mechanics to performance and confidence.
This integrative approach is not simply additive; it is transformative because it reframes rehabilitation from a checklist of impairments to a lived experience of growth. The modalities themselves reflect a shared ethic: care is client-centered, goal-driven, and contextual. The therapist’s stance is not merely to fix a problem but to collaborate with the person in shaping a pathway that honors values, daily routines, social roles, and personal aspirations. This requires a careful balancing act: the clinician must respect autonomy while offering expert guidance, push for functional gains while maintaining safety, and blend science with empathy. The clinical landscape recognizes that medical recovery cannot be reduced to numbers on a chart; it must be experienced in the rhythms of home life, social interaction, and meaningful work.
The theoretical and practical foundations of OT and PT are reinforced by professional standards that emphasize education, evidence-based practice, and ethical accountability. The WFOT articulates a global framework in which occupational therapy education includes rigorous clinical training and competencies that prepare practitioners to address physical, cognitive, sensory, and psychosocial dimensions of disability. In many parts of the world, including China, institutions align curricula with WFOT benchmarks, ensuring that graduates are equipped with neurorehabilitation knowledge, psychosocial considerations, and advanced technologies that support functional independence. This alignment highlights the shared global aspiration in rehabilitation: to ensure that everyone, regardless of background, has access to interventions that enable participation in daily life and community life. The standards are not self-contained requirements; they are signals of a field’s commitment to quality, accountability, and continuous improvement.
The synergy of OT and PT takes center stage in the story of rehabilitation across settings. In hospital wards, clinics, schools, workplaces, and homes, the two disciplines meet at the thresholds where pain is acknowledged and movement is reimagined as a pathway to participation. The clinical practice becomes a dynamic dialogue that moves with the patient’s changing needs. A patient may first demonstrate improvement in mobility, then gradually reveal the daily tasks that demand more nuanced control and strategy. An OT session might involve practicing meal preparation with adaptive equipment, while a PT session builds leg strength and balance to support stable standing posture. The transition from hospital to home is where this collaboration shines; it is where the patient’s independence becomes the organizing principle of ongoing care. The concept of moving “from hospital to home, from dependence to independence” is not merely aspirational rhetoric but a practical aim that shapes discharge planning, caregiver training, and community reintegration.
Technology has proliferated as a force multiplier in both OT and PT. The integration of digital tools, biofeedback, robotics, and 3D-printed assistive devices expands the toolkit available to clinicians and clients alike. Upper-limb exoskeletons, assistive devices for self-care, and therapeutic games that merge cognitive and motor challenges exemplify how technology can bridge gaps between impairment and function. However, technology is not a substitute for human-centered practice. It amplifies the clinician’s ability to tailor interventions to the person’s environment, preferences, and evolving goals. This person-centered, technologically enhanced approach is crucial when addressing long-term outcomes. A remarkable strength of OT and PT lies in their adaptability: the kind of therapy one person needs is rarely identical to another’s, and the environment in which care occurs constantly shifts, from acute care to community-based rehabilitation.
Across populations, the OT/PT partnership addresses a broad spectrum of needs. In stroke rehabilitation, the phases of recovery span motor re-acquisition, cognitive recalibration, and the restoration of everyday routines. In spinal cord injury, OT helps establish independence in essential tasks while PT rebuilds or compensates for sensorimotor pathways to reestablish safe function. For children with cerebral palsy or developmental differences, OT supports fine motor development, self-regulation, and school participation, while PT emphasizes motor planning, strength, and mobility. In geriatric care, both practices converge to maintain safety, preserve autonomy, and reduce the risk of secondary complications. Even in psychiatric and cognitive health contexts, OT brings a unique lens by integrating coping strategies, environmental adaptations, and meaningful activities that contribute to recovery, while PT contributes through movement-based interventions that reduce physical barriers to participation. The figures intersect with everyday life, underlining a fundamental truth: rehabilitation is about enabling a person to live the life they value, not merely to repair a body part.
For readers seeking a deeper sense of how OT and PT relate to one another and to broader health goals, the literature offers nuanced comparative perspectives. A widely discussed topic is the relationship and differences between OT and PT, including how they complement one another in practice. This conversation invites a careful look at what each discipline emphasizes and how clients experience care when both are involved. A thoughtful, balanced exploration can be found in discussions that compare the roles, goals, and outcomes of occupational therapy and physical therapy. See also the nuanced comparison of OT and PT in the blog post “occupational-therapy-vs-physical-therapy.” This internal resource provides a practical lens through which clinicians, patients, and families can appreciate the shared aims and distinct contributions of each profession while staying focused on meaningful participation and safe, effective movement. https://coffee-beans.coffee/blog/occupational-therapy-vs-physical-therapy/.
In sum, the foundations of OT and PT rest on a shared conviction: health emerges when people can engage in the activities that give their lives meaning. OT centers the person’s daily life, ambitions, and environment, translating capacity into participation. PT anchors recovery in movement, strength, and function, translating impairment into safe, efficient action. When combined, they form a holistic framework that bridges clinical improvement and real-world living. The true measure of success in rehabilitation is not only the restoration of a range of motion or a motor test score but the reentry into the world of human activity — the daily rituals, social participation, and purposeful work that define a life well lived. It is a pathway that respects the patient’s story, honors the realities of daily life, and remains open to innovation as the field evolves, always with the person at the center of care. For clinicians, students, and patients alike, this integrated model offers a map: a map that guides the journey from initial impairment toward a future of independence and dignity. The journey is ongoing, but with OT and PT as complementary guides, it becomes a navigable, hopeful process rather than a solitary, uncertain experiment.
External reference: WFOT provides the authoritative global definitions and principles that underpin this practice framework: https://www.wfot.org/what-is-ot/.
Bridging Movement and Meaning: The Integrated Practice of OT and PT in Modern Rehabilitation

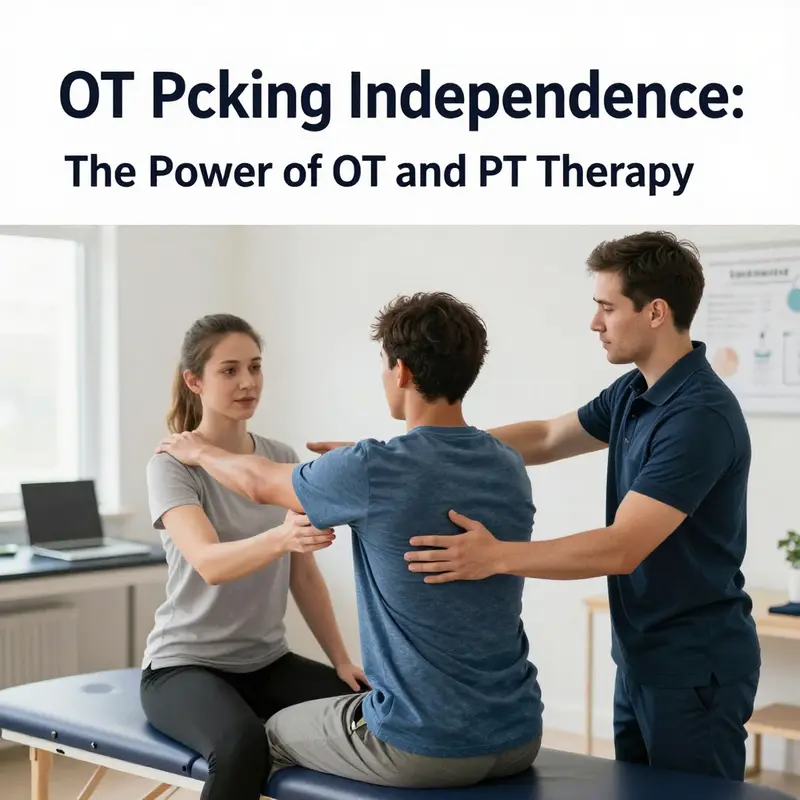
Two pillars stand at the core of rehabilitation medicine, interlocking to form a complete picture of recovery: physical therapy (PT) and occupational therapy (OT). They are not rivals but partners, each addressing a different, essential layer of the human experience after injury, illness, or disability. PT tends to lead with the body—restoring movement, strength, and the capacity to navigate the world with less pain and more control. OT, in contrast, tends to lead with function—rebuilding the everyday life that makes movement worthwhile, from dressing and cooking to managing finances and sustaining social connections. When these two approaches work in concert, the result is a patient who does not simply move again but can return to a life that feels whole, participatory, and dignified. The choreography between PT and OT grows from a shared respect for the body and a shared belief in the central aim of rehabilitation: to enable people to live as independently and meaningfully as possible, wherever they are on the recovery journey.
In the clinical landscape, PT is anchored in movement—the science of how joints, muscles, and nerves collaborate to produce patterns of motion that are efficient, safe, and adaptable. Its toolkit is rich with exercise therapy and physical agent modalities. Exercise therapy moves along a continuum from passive movements that preserve range of motion when a patient cannot initiate action, to active-assisted movements that nurture motor relearning, through to fully autonomous active movements that build strength, endurance, balance, and coordination. The essence of this progression is motor recovery: the brain’s capacity to relearn the maps that govern movement, synapses that rewire after a stroke or spinal injury, and the body’s tissues that heal in response to graded challenges. PT also employs a spectrum of physical agents—electrical stimulation, heat, cold, ultrasound, and biofeedback—to modulate pain, reduce inflammation, and reinforce neural and muscular activation. Within this framework, the body becomes a dynamic system in which neurons and muscles adapt in response to targeted, measurable stimuli.
OT complements this by translating regained capacity into practical, everyday use. Its core premise is not merely to “do a task” but to “learn through doing” tasks that matter in daily life. OT practitioners emphasize activity-based, goal-oriented engagement that reflects the patient’s own priorities and contexts. Their interventions span essential self-care activities like dressing, feeding, bathing, and toileting; instrumental activities of daily living such as cooking, laundry, and managing medications; and more complex tasks that enable a return to work or school, or to a community life that feels socially meaningful. Fine motor skills and hand function—critical for manipulating utensils, writing, typing, or operating a smartphone—receive careful attention. OT also addresses cognition, perception, and sensory processing, recognizing that memory, attention, problem-solving, and the way a person interprets sensations profoundly shape how one performs tasks. The therapeutic gaze shifts from the body’s raw capabilities to the person’s lived life, including the social, environmental, and psychological contexts that frame how well someone adapts to new limitations or new possibilities.
This dual focus is not a sequence but a seamless loop. A patient who has had a stroke may begin with PT to rebuild standing balance and leg strength, with the goal of standing safely at the sink or stepping to a chair. But recovery doesn’t stop at standing; OT picks up where PT leaves off, teaching safe self-care in the bathroom, enabling independence with meal preparation, and guiding the patient to organize a living space that reduces cognitive load and prevents falls. In spine rehabilitation, PT might focus on stabilizing the spine, restoring range of motion, and retraining gait. OT then helps adapt the home and workplace, ensuring that tools and routines support ongoing independence—whether that means designing a kitchen setup that minimizes reaching or teaching strategies to manage fatigue during daily routines. In pediatric contexts, PT supports motor milestones such as rolling, crawling, or walking, while OT focuses on the child’s ability to manipulate small objects, engage in classroom tasks, and participate in social play. Across ages and conditions, the two therapies meet at a shared goal: to transform recovery from a clinical achievement into a practical, daily reality that preserves dignity and purpose.
A practical way to appreciate their convergence is to imagine rehabilitation as a journey from hospital to home and into community life. PT equips travelers with trainable routes—the motor patterns and physical capacities needed to move through space with confidence. OT equips travelers with maps for navigating daily life—understanding how to prepare meals with adapted tools, how to dress in a manner that preserves energy, how to communicate effectively, and how to organize a day so that tasks align with fluctuating stamina and cognitive load. The journey is not a straight line but a circuit of reassessment, adaptation, and reinforcement. As patients regain movement, therapists monitor progress with standardized and individualized outcome measures, ensuring that improvements translate into real-world function. The patient’s goals—return to work, resume caregiving, participate in community activities, or simply perform self-care without excessive effort—anchor the rehabilitation plan. When PT and OT collaborate, goals become multidimensional and more closely aligned with what matters to the person living the day-to-day—the sense of control over one’s body, the assurance of safety in the home, and the social connectedness that makes daily life rewarding.
The rationale for this integrated approach is grounded in both science and lived experience. Neuroscience illuminates the brain’s remarkable capacity to reorganize itself after injury. Motor learning theories describe how practice conditions, feedback, and task-specific challenges shape the relearning of movement. OT expands this science into the realm of meaningful practice—tasks that patients perceive as relevant to their identities, roles, and futures. By embedding therapeutic activities within the fabric of daily life, OT turns rehabilitation into an empowering process rather than a sequence of isolated exercises. PT, by anchoring interventions in progressive loading, posture, proprioception, and neuromuscular coordination, provides the physiological substrate for renewed function. When these threads are woven together thoughtfully, recovery becomes a holistic enterprise: movement with purpose, purpose manifested in daily capability, and daily capability reinforced through ongoing participation in family, work, and community life.
A pervasive thread across settings is the emphasis on safety, independence, and prevention. PT contributes to fall prevention through balance training, functional sequencing, and strength work that stabilizes joints and enhances reaction times. OT extends safety into the home and community by evaluating environmental risks, selecting adaptive devices, and choreographing routines that reduce fatigue and cognitive overload. The goal is not to create dependence on a therapist or on assistive technology, but to cultivate a sustainable independence that patients can maintain beyond rehabilitation sessions. This balance—where support diminishes as competence grows—reflects a human-centered philosophy: therapy should empower resilience rather than foster reliance.
Another layer of integration lies in cognitive and psychosocial dimensions. OT’s attention to cognitive function and mental health threads through everyday tasks, helping patients build executive skills such as planning, prioritizing, and problem-solving. Whether a stroke survivor is regaining the initiative to manage appointments, or a young adult with a neurological injury is rebuilding a daily schedule, these cognitive competencies support confidence in performing tasks independently. PT’s role, too, recognizes psychosocial factors; motivation, persistence, and self-efficacy influence how consistently a patient adheres to a home exercise program or a home modification plan. The collaboration, then, becomes not just about physical tasks but about sustaining a hopeful narrative for life after illness or injury. In practice, therapists frequently co-create goals with patients, translating broad recovery aims into concrete, measurable milestones that reflect both movement and function in a real-world setting.
The landscape of interventions is vast, yet the throughline remains steady: therapy is most effective when it honors the person’s goals, respects their environment, and adapts to changing capabilities over time. PT’s robust repertoire of exercises, gait training, and neuromuscular reeducation sits alongside OT’s precision in hand function, cognition, and environmental adaptation. The synergy is visible in everyday examples. A patient learning to climb stairs after a spinal injury benefits from PT-driven leg strength and balance, but the day-to-day confidence to ascend safely also depends on OT-guided home modifications—handrails, lighting, and organized cues that reduce missteps. A teenager returning to sports must not only rebuild shoulder range of motion but also relearn how to perform school tasks, manage equipment, and navigate social dynamics that accompany athletic participation. In each case, the path to independence requires both the construction of robust movement and the cultivation of functional independence in daily life.
The integration of OT and PT is also a practical matter of clinical workflow and patient experience. Coordinated care plans reduce fragmentation, ensure consistency in messaging, and streamline patient expectations. When PT and OT share assessments and goals, they can sequence interventions so that motor gains translate into functional competence with minimal delay. Communication among the therapists—and with the patient and family—ensures that progress in movement aligns with improvements in self-care, home management, and social participation. The patient’s voice remains central: therapists continually ask what matters most, what is feasible in the living environment, and how improvements in one domain affect others. An informed, patient-centered approach makes rehabilitation coherent rather than episodic, turning episodes of treatment into a continuous story of adaptation, learning, and growth.
The evidence base for OT and PT supports this integrated model. Research highlights how task-specific training, repeated practice, and real-world applications produce meaningful gains in both movement and daily life. The literature emphasizes that outcomes are strongest when interventions are tailored to the individual’s goals and contexts, rather than when they are standardized across all patients. As clinicians reference guidelines and accumulate experience, they refine their ability to balance intensity with safety, to choose interventions that are enjoyable and engaging, and to pace progress in a way that respects the patient’s rhythms. It is this blend of science, craft, and personalized care that defines modern rehabilitation. For readers curious about the broader methodological landscape, a foundational overview of therapy interventions and approaches can be found in widely available clinical resources. the difference between physical therapy and occupational therapy offers a concise lens on how these disciplines complement one another and why their collaboration matters for patient outcomes. This perspective underscores that rehabilitation is not a single skill but a constellation of practices that, when aligned, empower the whole person to move through life with greater ease and dignity.
Ultimately, the story of OT and PT is a story about value—value not merely in restored muscle tests or improved gait, but in regained autonomy, meaningful participation, and the capacity to pursue what truly matters to a person’s life. When therapists design programs that honor the patient’s daily routines, social roles, and personal aspirations, they honor the essence of rehabilitation: to help people transform their experiences of dependency into opportunities for agency. The two disciplines, working together, illuminate a pathway from hospital walls to the thresholds of home and community. They remind us that healing is not only a matter of joints and nerves but of purpose—the chance to prepare a meal without excessive effort, to dress before sunrise, to engage in conversations with friends, to return to work, or to participate in play and learning with children. In these moments, therapy transcends technique and becomes a living practice of support, encouragement, and belief in the human capacity to adapt and thrive. The integrated OT-PT model thus stands as a compelling blueprint for holistic rehabilitation—one that honors both movement and meaning, and one that holds the promise of more complete, resilient, and authentic recovery for patients across the lifespan.
External resource: https://www.ncbi.nlm.nih.gov/books/NBK549807/
From Team Huddles to Daily Living: How Interdisciplinary OT and PT Care Shapes Real-World Recovery
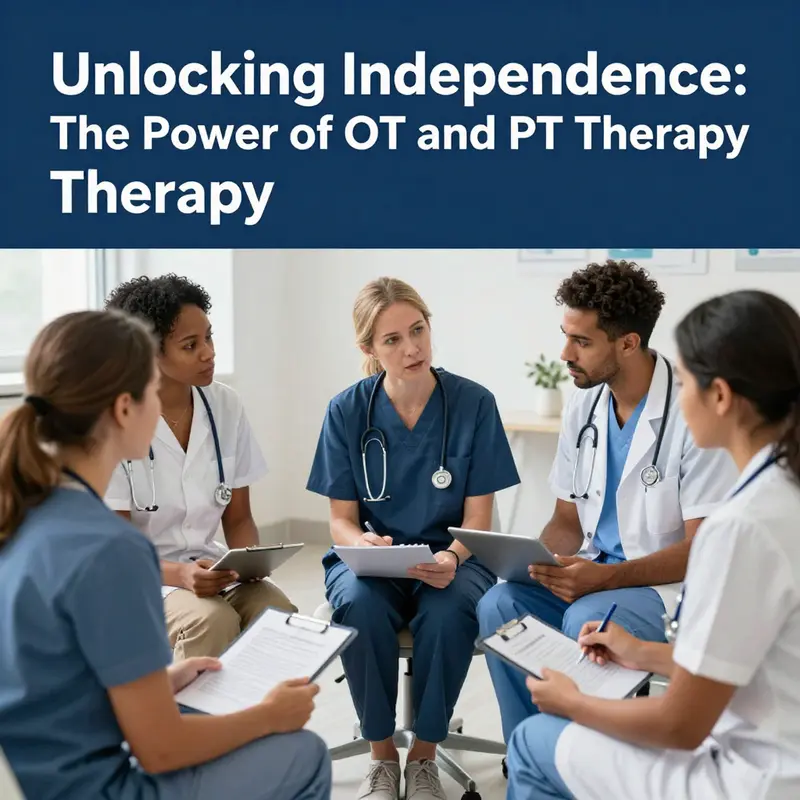
Across modern rehabilitation, occupational therapy and physical therapy do not simply operate side by side. They act as interwoven strands of a single therapeutic braid, each strengthening the other to restore a person’s capacity to live and engage with the world. The clinical logic is straightforward yet profound: improve what you can do now, while expanding what will be possible tomorrow. When OT and PT intersect with nursing, speech-language pathology, psychology, and social work, the result is not a series of isolated interventions but a cohesive patient-centered trajectory. This chapter examines how interdisciplinary collaboration translates into tangible outcomes, what makes the collaboration work in daily practice, and how evolving models of care further enhance recovery journeys from hospital corridors to home and community life.
The most compelling argument for integrated OT-PT care lies in the lived experience of patients who navigate complex, dynamic rehabilitation needs. A person recovering from a spinal cord injury, for example, faces a constellation of challenges: motor control, balance, pain modulation, cognitive clarity, mood fluctuations, and social participation. PT tends to prime the body for movement, strength, and endurance. It reconditions neuromuscular pathways, reduces pain, and rebuilds the capacity for ambulation or transfer. OT, by contrast, centers on meaningful activities—how a patient performs self-care, manages the environment, and re-engages roles such as parent, worker, or student. The synergy is not reductive; it is catalytic. PT creates a platform of bodily capability, and OT translates that platform into everyday independence. When these gains are pursued in concert, progress is more coherent, faster, and more durable.
In practical terms, this collaboration begins with an integrated assessment conducted by a multidisciplinary team. Yet the true strength emerges when professionals continue to align goals, monitor progress, and adjust plans in a shared, transparent manner. Regular team meetings become the heartbeat of care. They are not mere administrative rituals; they are dynamic forums in which clinicians review objective data, patient-reported experiences, and environmental factors. During a typical case conference, PT can report improvements in gait speed or sit-to-stand endurance, while OT highlights independence in dressing, meal preparation, or using adaptive equipment. The nurse contributes vital information about the patient’s medical stability, skin integrity, nutritional needs, and energy fluctuations. Speech therapists can illuminate communication and cognitive strategies, and a psychologist may address motivation and coping. Social workers help navigate home environments, community resources, and caregiver support. The cumulative effect is a care plan that speaks to the whole person, not just to isolated impairments.
One of the most powerful consequences of this systems-level thinking is the acceleration of functional recovery and the reduction of hospital stay. When OT and PT work with engineers of care—nurses, social workers, and therapists from other disciplines—patients begin to see a cascade of small but meaningful wins. A patient who learns to don a shoe and sock independently after a stroke may simultaneously retrain balance strategies with PT, enabling safer transfers and fewer fall risks. The same patient, supported by OT, might master meal prep with adaptive techniques, gradually reclaiming autonomy in the kitchen. As these daily-life competencies accumulate, the patient’s confidence grows, reducing dependency on external assistance and enabling a return to familiar roles. This dynamic also benefits the health system. Shorter hospital stays, fewer complications such as pressure injuries or deconditioning, and smoother transitions to home or community-based programs translate into tangible cost savings and improved overall outcomes.
Crucial to these improvements is the clarity of shared goals. When team members invest time in jointly defining patient-centered outcomes, the treatment plan remains anchored to what matters most to the person and their family. Goals are not static; they evolve as the patient progresses and as living contexts shift. For instance, early rehabilitation may emphasize basic self-care tasks and safe mobility, while later phases target community re-entry, return to work, or school activities. The team continuously revisits goals for feasibility, relevance, and timing. This dynamic process keeps therapy grounded in real life, ensuring that improvements in the clinic translate into meaningful changes at home, in the workplace, and within social networks.
The mechanisms that make interdisciplinary collaboration effective extend beyond shared goals. Communication is the central pillar, but it must be precise, timely, and bidirectional. In practice, this means standardized documentation, common outcome measures, and interoperable electronic records that enable all members of the team to view progress, flag concerns, and coordinate adjustments. It also means cultivating a shared language that transcends professional jargon. When a PT describes a patient as having “improved endurance,” and an OT translates that into the patient’s ability to complete a full meal preparation cycle, the care plan becomes more tangible for the patient and their family. This mutual intelligibility reduces confusion, aligns expectations, and fosters trust in the rehabilitation process.
Shared assessment tools play a pivotal role in ensuring consistency and comparability across disciplines. By using a common battery of functional measures, clinicians can track progress over time, identify plateaus, and signal when a shift in strategy is warranted. For the patient, seeing objective improvements—a longer distance walked, finer motor control in the hands, or quicker completion of daily tasks—provides motivational feedback and reinforces adherence to therapy plans. The literature increasingly supports the use of integrated evaluation frameworks, which help teams quantify the impact of OT and PT on broader outcomes such as daily activity performance, social participation, mood, and quality of life. In other words, the scorecards are not just numbers; they are stories of regained independence that the patient can share with caregivers, employers, and educators.
The case of spinal cord injury illustrates how interdisciplinary care can compress the timeline to meaningful independence. Immediately after injury, the focus is stability and preventing secondary complications. PT begins to reintroduce movement within safety limits, while OT teaches safe self-care routines and environmental modifications. As medical stability improves, the team collaborates to transition from acute care to rehabilitation wards and eventually to home-based programs. Each milestone—sitting balance, transfers to a chair, autonomous feeding, home safety assessments—becomes a joint accomplishment. The involvement of nursing ensures that medical risk factors are managed promptly, such as autonomic regulation or skin integrity, while social work plans for home adaptation and caregiver training. The cumulative effect is a rehabilitation arc that feels coherent to the patient: from immobilization to purposeful movement, from dependence to deliberate independence, and from hospital routines to personal autonomy in daily life.
This integrated approach is not limited to spinal cord injuries. Stroke survivors, patients with hip or knee replacements, individuals with arthritis, and even younger patients recovering from traumatic injuries all benefit from a coordinated OT-PT pathway. In pediatric and adolescent populations, the collaboration often extends to educational and developmental goals. OT can align self-care skills with school-based activities, while PT addresses posture, motor planning, and endurance needed for classroom participation and play. In these contexts, the family and school environment become essential partners in care, and the team’s flexibility to adapt settings—home, clinic, school, community centers—takes on heightened importance. The patient’s living environment, whether urban apartment or rural home, invariably influences the choice of interventions, assistive devices, and the pacing of recovery. The team’s ability to tailor interventions to real-world settings underlines the practical value of interdisciplinary collaboration.
To translate collaboration into durable outcomes, teams must address real-world barriers with creative strategies. Scheduling constraints, varied professional cultures, and differences in documentation practices can impede smooth teamwork. Successful programs implement structured yet flexible communication channels, such as daily brief check-ins, standardized handover notes, and shared dashboards that track functional milestones. They also invest in joint training that builds mutual respect and knowledge about each discipline’s methods, successes, and limitations. When clinicians understand each other’s rationale, they can harmonize therapy plans even when a patient’s condition shifts or when resources become limited. The cultural shift toward patient-centered care further reinforces collaboration. Teams that invite patient and family input in setting goals, choosing strategies, and signaling acceptable trade-offs tend to achieve higher engagement, stronger adherence, and more satisfying outcomes for all involved.
Evidence from contemporary rehabilitation literature points to broader benefits of such collaboration beyond individual patients. Interdisciplinary models have been associated with improved functional recovery, higher levels of daily life participation, reduced caregiver burden, and more efficient use of healthcare resources. The value is not merely additive but synergistic; OT and PT, working within a well-integrated team, create a ripple effect that touches nutrition, mental health, community reintegration, and long-term wellness. When care becomes a shared responsibility among professionals, patients experience continuity of care that sustains gains achieved during therapy and supports ongoing self-management after discharge. In an era when chronic disease and aging populations place increasing demands on health systems, such collaborative models are central to delivering high-quality, cost-conscious rehabilitation.
For readers seeking a concise synthesis of how these practices translate into clinical workflows, a practical overview of collaboration across health care teams is available at how do occupational therapists collaborate with other healthcare professionals. This resource outlines core strategies—shared goals, common assessment frameworks, coordinated care planning, and patient-centered communication—that undergird successful rehabilitation. The aim is not to replace discipline-specific expertise but to fuse it into a coherent care experience that centers on the patient’s life as it unfolds outside therapy sessions. The end goal remains simple yet aspirational: empower individuals to perform the tasks that matter most to them, with the confidence that their care team stands with them at every step.
Looking forward, advances in technology and new care-delivery models are likely to expand the reach and effectiveness of interdisciplinary OT-PT care. Tele-rehabilitation, remote monitoring of activity, and digital platforms for goal tracking can support continuous collaboration even when patients transition to home environments or community programs. These tools help maintain accountability, preserve momentum, and enable families to participate more actively in the rehabilitation process. Yet technology alone cannot replace the human elements of collaboration—the trust, empathy, and shared purpose that emerge when professionals from diverse backgrounds come together with a single patient-centered mission. The science is clear that when teams communicate well, align goals, and coordinate interventions, patients regain independence more quickly, live with better quality of life, and participate more fully in social and occupational roles. The challenge lies not in proving that collaboration works, but in designing care systems that make it feasible, scalable, and sustainable across varied settings and populations.
External resource for broader context: https://www.sciencedirect.com/topics/medicine-and-dentistry/interdisciplinary-collaboration
Toward a Living Bridge: Future Directions and Innovations in OT and PT Therapy
The future of occupational therapy (OT) and physical therapy (PT) is less a catalog of new devices and more a reimagining of care as an integrated, adaptive journey from hospital to home, and sometimes beyond. It is a narrative that centers on people—how they live, how they adapt, and how technology can extend their independence without eroding the human relationship at the heart of healing. In this chapter, we explore where OT and PT are headed, not as isolated disciplines but as complementary, evolving forces designed to meet a changing world. We begin with the digital turn that is already reshaping practice, then move to broader commitments around accessibility, scope, and collaboration that will define care in the years ahead. It is a future defined by patient-centered outcomes, data-informed decision making, and a philosophy that rehabilitation is not merely about restoring movement or task performance but about reclaiming meaningful participation in daily life. As such, the direction is both practical and aspirational, rooted in the realities of today’s health systems while imagining what could be possible when clinicians, patients, families, and communities share a common language of recovery.
The most immediate transformation in OT and PT is digital competence. Telehealth, remote assessment, and virtual interventions have moved from experimental pilots to standard options in many care settings. For patients living in remote or underserved areas, digital platforms can remove a long journey to clinics while preserving timely, high-quality care. Yet the shift to virtual care is not a simple transfer of in-person practices to a screen. It requires rethinking evaluation methods, coaching strategies, and the cadence of sessions. What does a functional assessment look like when a therapist cannot palpate, but can observe, measure, and prompt using real-time data? How can therapists gauge subtle changes in motor control during a home exercise program without hands-on feedback? These questions underscore the necessity of new communication techniques, user-friendly interfaces, and clear, task-oriented feedback mechanisms that translate movement quality into actionable guidance. At the same time, digital platforms enable continuous monitoring that can detect early warning signs of decline or plateau, triggering timely adjustments to therapy plans. The result is a more responsive, adaptive form of care that respects patients’ time and preferences while expanding access.
Accessibility and inclusivity sit at the core of these innovations. The promise of OT and PT rests on the assurance that diverse populations—varying in culture, language, education, age, socioeconomic status, and disability—can engage with care on their own terms. This means tailoring assessment tools, intervention materials, and communication styles to fit individual contexts. It also means taking up the challenge of cognitive and sensory differences in a respectful, strength-based manner. The shift toward inclusive practice requires ongoing collaboration with patients and families to co-create goals that are meaningful in real life. It invites communities to participate in care planning, thereby strengthening social support networks that reinforce rehabilitation gains. In practical terms, this translates to designing home programs that fit a patient’s daily routine, creating culturally resonant activity choices, and ensuring that digital solutions are accessible to people with limited literacy or sensory impairments. The overarching aim is not merely to deliver care but to build environments—homes, schools, workplaces, and neighborhoods—that sustain recovery. Such environments become extensions of the therapeutic plan, where the patient’s daily actions at home become therapeutic opportunities and the person’s social world reinforces resilience.
Expanding the scope of practice is the second axis of future progress. OT and PT are increasingly stepping into proactive roles in preventive care and chronic disease management. This shift reflects a broader shift in health systems toward keeping people well and functioning in the community rather than primarily treating illness in specialized settings. Therapists are engaging in population health models, contributing to program design for fall prevention in aging populations, promoting activity and energy conservation for individuals with long-term conditions, and collaborating on cognitive and psychosocial strategies that support sustained participation in work and school. Interdisciplinary collaboration becomes not just a virtue but a necessity as complex patients demand coordinated plans spanning primary care, neurology, orthopedics, mental health, and social services. The ability to connect therapy goals with broader health outcomes—like reduced hospital readmissions, improved self-management of chronic diseases, and enhanced quality of life—becomes a core metric of success. This expanded scope invites therapists to assume roles in health education, home safety modification, ergonomic coaching, vocation rehabilitation, and community-based activity programming. The result is a more proactive profession, where prevention and timely intervention are integrated into the DNA of daily practice, rather than treated as optional add-ons.
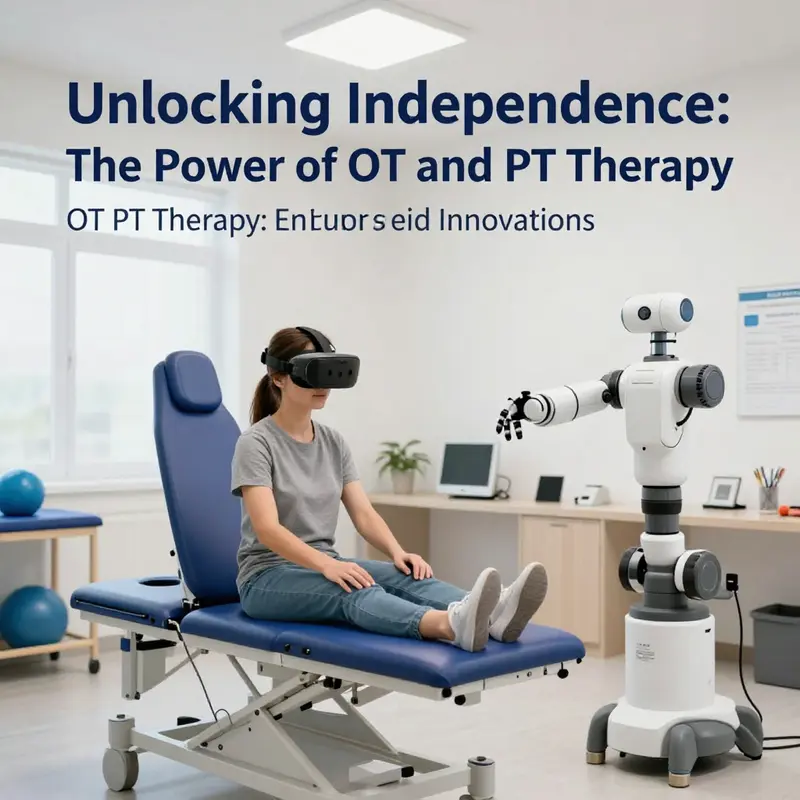
Innovations in OT and PT will be shaped by three interlocking technologies: wearable devices, artificial intelligence (AI), and data-driven decision tools. Wearables offer real-time insight into movement patterns, posture, gait quality, and daily activity levels. When combined with patient-reported outcomes and clinical observations, wearables help therapists tailor interventions with unprecedented granularity. The challenge lies in translating the continuous stream of data into meaningful decisions without overburdening clinicians with information or patients with surveillance anxiety. AI and machine learning can sift through diverse data sources to identify patterns, predict response to therapy, and personalize treatment plans. These capabilities promise to move care toward precision rehabilitation: an approach where exercises, progression criteria, and assistive strategies are matched to the individual’s biology, environment, and life goals. Importantly, these tools should augment the clinician’s judgment, not replace it. They should support transparent decision making, enabling patients to understand why a particular course of action is recommended and how it aligns with their values and daily routines.
Data-driven decision making offers both promise and responsibility. Real-time progress tracking enables therapists to respond quickly to plateaus or setbacks, adjusting intensity, volume, or strategy while maintaining patient engagement. Predictive analytics can help identify patients at risk of relapse or decline after discharge, guiding the design of post-therapy maintenance plans and community supports. With such tools, the line between hospital and home becomes a continuum of care where decisions are anchored in objective data, yet always interpreted through the lens of the patient’s lived experience. The ethical dimension of this shift cannot be overlooked. Safeguards for privacy, consent, and data ownership are fundamental. Clinicians must ensure that data collection enhances autonomy rather than compels or restricts it. Moreover, the deployment of advanced tools should be accompanied by ongoing education for clinicians, ensuring they are proficient in both the technical and human implications of data-driven practice. As the field evolves, curricula and continuing education should incorporate digital literacy, data ethics, and patient communication in the digital age, equipping therapists to navigate evolving responsibilities with confidence and compassion.
All these trends converge on a central premise: effective OT and PT care in the future will hinge on collaboration. Therapists will work side by side with bioengineers, data scientists, educators, employers, and policymakers to design care pathways that are scientifically sound and socially just. Interdisciplinary teams will align therapy goals with broader rehabilitation pathways, ensuring consistency across settings—from acute care to home modification, from school-based supports to workplace reintegration. The patient and their family will be partners in a shared decision-making process that respects preferences, clarifies trade-offs, and emphasizes sustainable independence. This is not a surrender to technology but an invitation to harness it for greater humanity in care. A digitally enhanced OT/PT practice can deliver more precise assessments, more engaging interventions, and more reliable follow-through, all while preserving the central human qualities that define therapy—the empathy to listen, the patience to guide, and the expertise to tailor interventions to a person’s unique life story.
Within this evolving landscape, the clinician’s role remains both art and science. The art lies in interpreting movement and function through a holistic lens, recognizing that a change in mobility often signals shifts in mood, cognition, or social participation. The science lies in applying evidence-based protocols, validating new approaches, and continually refining techniques in response to patient feedback and outcome data. The future OT/PT practitioner will be adept at blending soft skill with data-driven strategies, translating numbers into meaningful, actionable advice that patients can embrace. The success of such a combined approach rests on trust: trust in the therapist’s expertise, trust in the technology that supports care, and trust in the patient’s agency to pursue a path that reflects their values and aspirations.
As we look toward implementation, several practical considerations surface. Reimbursement models must adapt to support flexible, remote, and home-based care without compromising quality. Training infrastructures should provide clinicians with hands-on experience in digital tools, remote communication tactics, and culturally responsive care delivery. Policy makers and administrators will need to champion scalable solutions that reduce disparities rather than widen them, ensuring that innovations reach those who stand to benefit most. Healthcare organizations can foster a culture of learning by embedding research into routine practice, encouraging clinicians to measure outcomes, test new approaches, and share findings in a way that accelerates collective progress. In this sense, the future of OT and PT therapy is also a future of healthier systems—sustainable, equitable, and responsive to the changing needs of society.
To illustrate how technology and collaboration can reframe patient care in practice, consider how a patient who has experienced a neurological event might engage with therapy. A PT might deploy wearable sensors to monitor gait symmetry and endurance during home walking tasks, while an OT tracks fine motor recovery and daily activity participation through smart home interfaces and adaptive equipment. Telehealth sessions serve as the primary touchpoint for review and coaching, with in-person visits reserved for hands-on assessments or equipment fitting. Throughout, the care team remains attentive to the patient’s goals—returning to meaningful activities, improving safety at home, re-engaging with school or work, and sustaining a sense of independence. The care plan evolves with the patient, shaped by quantitative data and qualitative feedback, reflecting a responsive partnership that honors patient autonomy and dignity. This is the envisioned synthesis of OT and PT: two disciplines, one patient-centered mission, and a continuous loop of learning, adaptation, and growth that extends beyond the clinic walls.
For readers seeking a deeper scholarly anchor for these trajectories, the broader conversation about extending physical therapist scope of practice to improve quality of care and preserve health system sustainability offers critical insights. While the chapter above centers on practical implications for OT and PT, it is worth noting the evidence that supports expanding professional capabilities within safe, rigorous boundaries. The referenced work in the Journal of Orthopaedic and Sports Physical Therapy provides an informed framework for understanding how scope advancement can align with improved care quality and system efficiency. This connection between clinical evolution and health system resilience is essential as the field moves toward more preventive and community-based models of rehabilitation.
In parallel with scholarly discourse, clinicians and educators can draw practical guidance from reflections on technology’s role in patient care in OT. A growing body of resources discusses how digital tools reshape evaluation, intervention, and outcomes measurement, offering case examples, best practices, and ethical considerations. Technology is not a cure-all; it is a powerful enabler when deployed thoughtfully, with attention to patient preferences, accessibility, and the preservation of therapeutic rapport. The future, then, is not merely about more devices or faster data streams; it is about crafting care that is more responsive, more inclusive, and more attuned to what matters most to people trying to live well with or beyond illness and disability. As this chapter suggests, the ultimate measure of progress lies in the degree to which therapy helps individuals reclaim meaningful participation, sustain independence, and experience a sense of agency in daily life.
For practitioners reading these lines, the path forward invites both courage and curiosity. Embracing telehealth, wearables, AI, and data tools requires skills, empathy, and a commitment to ethical practice. It also demands humility—the recognition that technology should serve human flourishing, not overwhelm it. With this orientation, OT and PT can continue to bridge the gap between clinical expertise and everyday living, transforming rehabilitation from a sequence of isolated sessions into a continuous, living process that carries people toward fuller, more resilient lives. The future is not predetermined; it is co-created by clinicians who adapt with intention, patients who participate with purpose, and systems that support sustainable, equitable care. In that shared venture, OT and PT therapy become more than disciplines. They become a living bridge—connecting science, compassion, and everyday possibility across the arc of recovery.
Internal link note: As technology becomes more integrated into care, nuanced conversations emerge about how to balance digital tools with human-centered approaches. A detailed discussion is available here: What role does technology play in enhancing patient care in occupational therapy?.
External resource for further reading: https://doi.org/10.1016/j.jopm.2018.05.004
Final thoughts
As we look towards the future of rehabilitation, the significance of Occupational Therapy and Physical Therapy cannot be overstated. These interwoven therapies not only enhance physical capabilities but also promote the essential skills needed for everyday living. Business owners in healthcare must recognize the importance of these collaborative approaches to improve patient outcomes and satisfaction. Adopting innovations and advanced treatment techniques will ensure that healthcare practices remain effective and responsive to the evolving needs of patients. By harnessing the strengths of OT and PT, we can pave the way for a new standard in rehabilitation that champions independence and enriches lives.